Introduction
Diagnosis of hypothalamic-pituitary-adrenal (HPA) insufficiency (HPAI) is challenging, and underrecognition of this disorder has serious consequences. Consequently, untreated secondary adrenal insufficiency (AI) is associated with increased mortality and morbidity [1]. Corticotropin, or adrenocorticotropic hormone (ACTH), regulates the function of the two inner layers of the adrenal cortex, the zona fasciculata and zona reticularis, which secrete glucocorticoids and adrenal androgens, respectively [2]. Corticotropin-releasing hormone (CRH) is a peptide hormone secreted by the hypothalamus. It is responsible for the secretion of ACTH by the pituitary gland. Based on this, measurement of plasma ACTH levels helps differentiate between primary and secondary AI. Cortisol and ACTH follow a circadian rhythm: cortisol reaches a maximum concentration in the early morning, between 6 and 8 a.m. [3]. However, in clinical practice, early morning basal cortisol is used to diagnose AI. A serum cortisol level below 1.8 μg/dL or above 18 μg/dL confirms and excludes, respectively, HPA insufficiency (HPAI) [4].
Adrenal androgens, such as androstenedione, dehydroepiandrosterone (DHEA), and DHEA sulfate (DHEA-S), are less influenced by circadian rhythm and the latter have a long half-life of 10-20 hours. This is especially true for DHEA-S [5]. Normal age- and gender-specific DHEA-S levels demonstrate a sensitivity of 100% for excluding HPAI [6]. Plasma ACTH is less commonly used in the diagnostic evaluation of HPAI in clinical practice because it is within the normal range or lags behind the suppression of cortisol and DHEA-S [7]. Dynamic tests remain the best way to diagnose endocrine diseases. In AI, the gold standard is the insulin tolerance test, also known as insulin-induced hypoglycemia. It is currently banned and not used in HPAI [8]. Instead, at present, the most common method for assessing HPAI is the short cosyntropin stimulation test. The limitations of performance are related to low specificity and sensitivity (only 57-79%) [9, 10]. Hence, more sensitive and specific methods for assessing HPA axis integrity are needed.
The goal of this study was to evaluate the performance of measuring serum cortisol, serum DHEA-S, and plasma ACTH levels vs. the standard short cosyntropin simulation test (the standard dose of 250 μg) for diagnosing HPAI.
Material and Methods
Normal reference intervals
Serum cortisol levels range from 5 to 25 μg/dL, while plasma ACTH levels range from 7 to 66 pg/mL, depending on the assay used. According to Mayo Clinic laboratories [11], reference intervals for serum DHEA-S levels depend on age and gender.
Normal and low values are defined as follows:
· Morning fasting test: normal cortisol ≥5 μg/dL, low cortisol <5 μg/dL;
· DHEA-S level: normal ≥ 50 μg/dL, low <50 μg/dL;
· Plasma ACTH level: normal ≥ 6 pg/mL, low <6 pg/mL;
· Short cosyntropin stimulation test: normal or negative ≥18.5-20 μg/dL; abnormal, dampened, or positive <18.5 μg/dL [12].
Setting and participants
We recruited the participants for this cross-sectional study from the FDEMC (Basra, Iraq) between November 2021 and October 2022.
In our study, we included patients with suspected HPAI, particularly those aged 15 years or older who were taking exogenous steroid medications intermittently or continuously for at least one month, or were experiencing symptoms and signs suggestive of AI, or unexplained symptoms such as weight loss, anorexia, and other gastrointestinal symptoms [13].
Exclusion criteria for the study were as follows:
· Patients referred from the intensive care unit (ICU);
· Current glucocorticosteroid therapy or replacement therapy within the previous week;
· Pregnant women, as well as those who have taken oral contraceptives or hormone replacement therapy within the previous six weeks;
· Drugs that affect cortisol metabolism, such as spironolactone and antiepileptic drugs;
· Primary AI (Addison’s disease);
· Patients who had undergone transsphenoidal surgery, had a history of trauma, radiation, or infection, or other structural pituitary diseases.
Based on the above criteria, we initially included 252 patients who underwent cortisol, DHEA-S, and ACTH testing on the same day if they were fasting, or were asked to return the following day for testing in a fasting state. To determine cortisol and DHEA-S, 2 mL of blood was collected and placed in a gel tube, and to determine ACTH, in an EDTA tube. If the results of either test were below the reference range (i.e., cortisol <5 μg/dL, DHEA-S level for certain age/gender and ACTH level <6 pg/mL), we asked participants to undergo a short cosyntropin stimulation test the following day, regardless of fasting: 2 mL of blood were placed in a gel tube, 250 μg of cosyntropin were then administered intramuscularly, and another 2 mL of blood were collected in a gel tube 30 minutes and 1 hour after the injection.
The total number of participants meeting the biochemical criteria for HPAI was 228. Of these, 196 were admitted to the short cosyntropin stimulation test, and the remainder were treated according to the protocol. Of the 196 participants, 27 did not complete the test; hence, the remaining 169 constituted the final sample of the study (Figure 1).
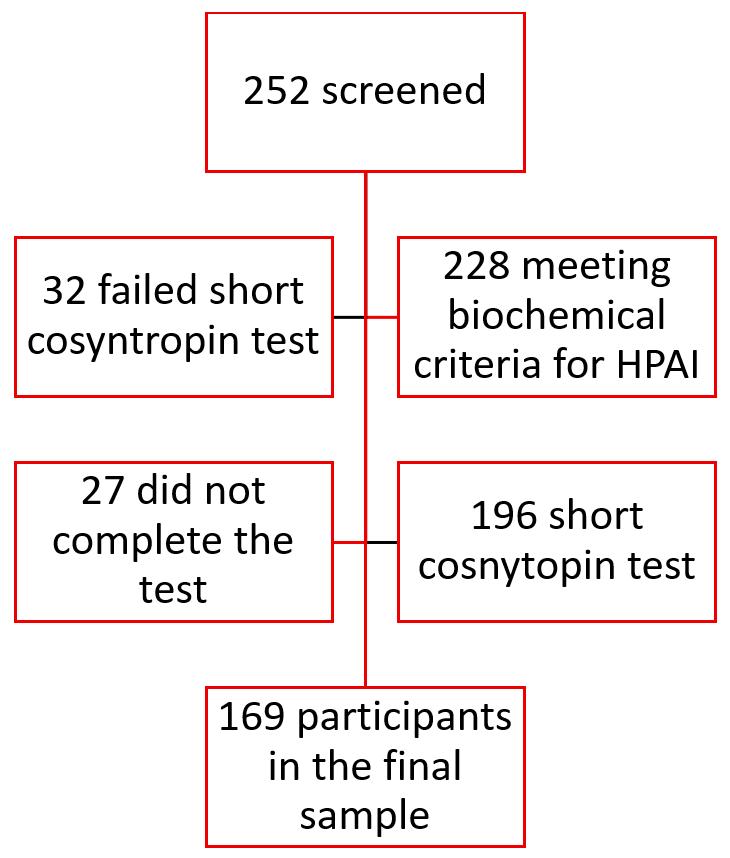
Figure 1. Algorithm for forming the research sample.
All study participants provided verbal informed consent, and the Ethics Committee of Basra College of Medicine approved the study protocol.
Biochemical analyses
All patients were given instructions the day before the procedure; fasting was not required. The procedure was performed between 9:00 and 11:00 a.m. A 10 mL blood sample was drawn from all patients to determine baseline cortisol, ACTH, and DHEA-S levels. All blood samples were serum, except for ACTH, which was measured in plasma. Then, 250 μg of cosyntropin was administered intramuscularly, and cortisol levels were measured at 0, 30, and 60 minutes. A normal adrenal reserve response is defined as a cortisol level greater than 18.0-20 μg/dL (500-555 nmol/L) at any time point, 30 or 60 minutes, or both.
Research instruments
Plasma ACTH, serum cortisol, and serum DHEA-S levels were measured using an electrochemiluminescence immunoassay (ECLIA) on a Cobas e411 analyzer (Roche Diagnostics, Germany) using the manufacturer’s reagents and instructions. For ACTH, the measurement range was 1.0-2,000 pg/mL, and the intra-assay precision was specified at 5-100 pg/mL, i.e., coefficient of variation (CV) <5%. For cortisol, the measurement range was 0.018-63.4 μg/dL, and the intra-assay precision was specified at >110 nmol/L (CV<6%). For DHEA-S, the measurement range was 0.100-1,000 μg/dL, and the intra-assay precision was specified at 50-1,000 μg/dL (CV<5%).
Statistical analysis
Data analysis was performed using the Statistical Package for the Social Sciences (SPSS) 15 (SPSS Inc., Chicago, IL, USA). Continuous variables are presented as mean and standard error of the mean (SE). Categorical variables are presented as percentages. The area under the receiver operating characteristic (ROC) curve was used to assess the diagnostic performance of each of the three parameters: plasma ACTH level, serum DHEA-S level, and serum cortisol level. Combinations of abnormal cortisol and ACTH levels (Panel I), abnormal DHEA-S and ACTH levels (Panel II), abnormal cortisol and DHEA-S levels (Panel III), and abnormal cortisol, DHEA-S, and ACTH levels (Panel IV) were used to predict abnormal short cosyntropin test results. Cutoff values for plasma ACTH, serum DHEA-S, and serum cortisol levels were calculated by plotting the true positive outcome (sensitivity) vs. the false positive outcome (1 – specificity).
Results
The cause of severe HPA syndrome, manifesting as AI in our patients, was exogenous glucocorticosteroid use in most patients or the presence of HPAI symptoms without a history of drug use. None of the participants in our study had a history of pituitary tumors, surgery, or radiation therapy. The total number of study participants was 169 patients (Table 1), of whom 134 (79.3%) were women. Although the age of the entire cohort ranged from 20 to 80 years, represented by a mean ± SEM of 38.8±0.94 years, the majority (77.5%) were in the age group of 21 to 50 years. ACTH levels were suppressed in 40% of patients, and within the reference range in 59.2%.
Table 1. Characteristics of the study participants
|
Variable |
No. (%) |
|
|
Male |
35 (20.7) |
|
|
Female |
134 (79.3) |
|
|
Age, years (Mean ± SE; range: 20-80) |
38.9±0.94 |
|
|
DHEA-S |
Normal (≥50 µ/dL) |
71 (42.0) |
|
Low (<50 µ/dL) |
96 (56.8) |
|
|
Missing |
2 (1.2) |
|
|
Cortisol |
Normal (≥5 µ/dL) |
102 (60.3) |
|
Low (<5 µ/dL) |
67 (39.7) |
|
|
ACTH |
Normal (≥6 pg/mL) |
69 (40.8) |
|
Low (<6 pg/mL) |
100 (59.2) |
|
|
Short cosyntropin test |
Negative (≥20 µ/dL) |
104 (61.5) |
|
Positive (<18 µ/dL) |
65 (38.5) |
|
The mean ± SE for ACTH was 28.6±11.8 pg/mL. DHEA-S level was 75.36±8.6 μg/dL; its level was low in 56.8% of patients. Basal serum cortisol level was 9.7±0.857 μg/dL; its level was low in 39.7% of patients. The short cosyntropin test results were abnormal in 65 patients (38.5%).
The tables below present the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of all parameters (plasma ACTH, serum DHEA-S, and serum cortisol) compared to the standard test (the short cosyntropin test).
The sensitivity of the plasma ACTH level was 68.8%, the specificity was 74.5%, the PPV was 62.9%, and the NPV was 79.2%. This translates into a false positive rate of 25.5%, a false negative rate of 31.2%, a true positive likelihood ratio of 2.92, and a true negative likelihood ratio of 0.418 (Table 2).
Table 2. Sensitivity and specificity of plasma ACTH vs. the short cosyntropin test
|
|
Positive (dampened) (<18 µ/dL) |
Negative (≥20 µ/dL) |
|
|
|
Plasma ACTH level |
Low (<6 pg/mL) |
43 |
26 |
62.9% PPV |
|
Normal (≥6 pg/mL) |
22 |
78 |
79.2% NPV |
|
|
|
68.8% Sensitivity |
74.5% Specificity |
|
|
|
Total |
65 |
104 |
||
The sensitivity of the serum DHEA-S level was 89.2%, the specificity was 62.7%, the PPV was 60.4%, and the NPV was 90.1%. This translates into a false positive rate of 37.3%, a false negative rate of 10.8%, a true positive likelihood ratio of 2.39, and a true negative likelihood ratio of 0.172 (Table 3).
Table 3. Sensitivity and specificity of serum DHEA-S vs. the short cosyntropin test
|
|
Positive (dampened) (<18 µ/dL) |
Negative (≥20 µ/dL) |
|
|
|
Serum DHEA-S level |
Low (<50 µ/dL) |
58 |
38 |
60.4% PPV |
|
Normal (≥ 50µ/dL) |
7 |
66 |
90.1% NPV |
|
|
|
89.2% Sensitivity |
63.4% Specificity |
|
|
|
Total |
65 |
104 |
||
The sensitivity of the serum cortisol level was 87.7%, the specificity was 90.4%, the PPV was 85.1%, and the NPV was 92.2%. This translates into a false positive rate of 9.6%, a false negative rate of 12.3%, a true positive likelihood ratio of 9.13, and a true negative likelihood ratio of 0.136 (Table 4; Figure 2).
Table 4. Sensitivity and specificity of serum cortisol vs. the short cosyntropin test
|
|
Positive (dampened) (<18 µ/dL) |
Negative (≥20 µ/dL) |
|
|
|
Cortisol level |
Low (<5 µ/dL) |
57 |
10 |
85.1% PPV |
|
Normal (≥5 µ/dL) |
8 |
94 |
92.2% NPV |
|
|
|
87.7% Sensitivity |
90.4% Specificity |
|
|
|
Total |
65 |
104 |
||
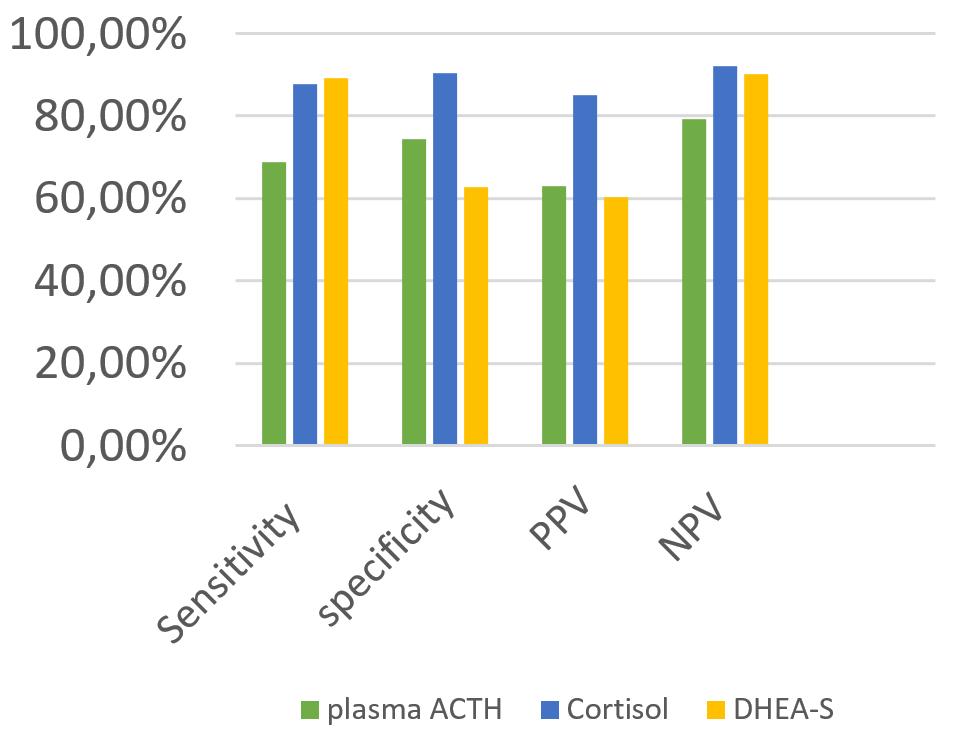
Figure 2. Sensitivity, specificity, PPV, NPV, and predictive values of different tests vs. the short cosyntropin test (ACTH, adrenocorticotropin; DHEA-S, dehydroepiandrosterone sulphate).
The serum cortisol cutoff values predicting an abnormal short cosyntropin test result were <5.31 μg/dL, with a maximum sensitivity and specificity of 87.7% and 90.4%, respectively. The DHEA-S cutoff values predicting an abnormal short cosyntropin test result were <31.11 μg/dL, with a sensitivity of 89.2% and a specificity of 62.7%. The least reliable parameter predicting an abnormal short cosyntropin test result was the plasma ACTH level, with a cutoff <5.30 pg/mL, and with the lowest sensitivity (68.8%) and specificity (74.5%) (Table 5).
Table 5. Cutoff values of serum cortisol, DHEA-S, and plasma ACTH and their predictive performance in indicating an abnormal short cosyntropin test result
|
Test |
The area under the ROC curve (95% CI) |
Cutoff value |
Sensitivity |
Specificity |
|
Plasma ACTH |
0.762 (0.679-0.834) |
5.30 pg/mL |
68.8% |
74.5% |
|
Serum DHEA-S |
0.887 (0.829-0.936) |
31.11 µg/dL |
89.2% |
62.7% |
|
Serum cortisol |
0.941 (0.903-0.979) |
5.31 µg/dL |
87.7% |
90.4% |
|
Cortisol (<5 µ/dL) and ACTH ( 6 pg/mL) (Panel I) |
0.775 (0.696-0.855) |
– |
60.0% |
95.1% |
|
DHEA-S (<50 µ/dL) and ACTH (<6 pg/mL) (Panel II) |
0.776 (0.697-0.855) |
– |
63.1% |
92.2% |
|
Cortisol (<5 µ/dL) and DHEA-S (<50 µ/dL) (Panel III) |
0.916 (0.863-0.969) |
– |
86.2% |
97.1% |
|
Cortisol (<5 µ/dL), DHEA-S (<50 µ/dL), and ACTH (<6 pg/mL) (Panel IV) |
0.795 (0.717-0.873) |
– |
60.0% |
99.0% |
Table 5 presents the comparison of baseline parameters with cosyntropin test results. The highest specificity and sensitivity for HPAI were observed with the combination use of basal morning serum cortisol and serum DHEA-S levels, reaching 86.2% and 97.1%, respectively. The only equivalent indicator was basal morning cortisol, with a specificity and sensitivity of 87.7% and 90.4%, respectively. Combining all parameters (serum cortisol, serum DHEA-S, and plasma ACTH levels) increases specificity to 99% but reduces sensitivity to a very low level (60.0%).
Using a combination of laboratory tests to improve the prediction of abnormal short cosyntropin test results shows that the joint use of morning serum cortisol and serum DHEA-S levels produces the best results.
In paired comparisons, morning cortisol level shows the best results in HPAI screening compared with ACTH and DHEA-S (p=0.005 and p=0.058, respectively) (Table 6). It ranks first among test combinations, as clearly demonstrated by the descriptive nonparametric Youden index (Youden’s J statistic) (Table 7).
Table 6. Pairwise comparison of ROC curves for ACTH, DHEA-S, and cortisol
|
Test |
AUC difference |
SE |
95% Confidence interval |
p-value |
|
Cortisol-DHEA-S |
5.80 |
21.6 |
2.0 -11.8 |
0.058 |
|
Cortisol-ACTH |
19.0 |
24.4 |
11.0-27.1 |
0.000 |
|
DHEA-S-ACTH |
13.2 |
26.1 |
11.8-22.5.0 |
0.005 |
Table 7. Assessing the performance of individual laboratory tests and their combinations using Youden’s J statistic
|
Test |
Sensitivity |
Specificity |
Youden’s J statistic |
|
Cortisol+ DHEA-S |
86.2 |
97.1 |
83.3 |
|
Cortisol |
89.2 |
91.2 |
80.4 |
|
DHEA-S |
95.2 |
66.3 |
61.5 |
|
Cortisol+ DHEA-S+ ACTH |
60.0 |
99.0 |
59.0 |
|
DHEA-S+ ACTH |
63.1 |
92.2 |
55.3 |
|
Cortisol+ ACTH |
60.0 |
95.1 |
55.1 |
|
ACTH |
67.7 |
75.5 |
43.2 |
ACTH, adrenocorticotropin; DHEA-S, dehydroepiandrosterone sulphate.
Discussion
Hypothalamic pituitary adrenal insufficiency (HPAI) is often partial, resulting from insufficient secretion of CRH and/or ACTH. This makes diagnosing HPAI quite challenging for many endocrinologists. Patients with partial ACTH deficiency show an unresponsive short cosyntropin stimulation test, especially if the cortisol cutoff value is ≤18.1 μg/dL. Using a cutoff value of 20 μg/dL increases sensitivity [10].
Adrenal insufficiency (AI) after discontinuation of glucocorticoids is common. There is no single type of steroids, dosage, duration of treatment, or indications for disease that can reliably exclude AI [13].
The use of over-the-counter glucocorticoids has been common in Iraq for many years, significantly increasing the risk of HPAI, especially if these medications are suddenly discontinued. Most cases of HPAI reported at FDEMC were linked to the use of exogenous corticosteroids, primarily those obtained over-the-counter. More than two-thirds of patients were women aged 21-50 years. A similar trend was previously observed at FDEMC, with women accounting for 69% of those self-prescribing corticosteroids [14]. Comparable findings have been reported worldwide [15].
The effectiveness of DHEA-S is moderate. A study has shown that a normal level of DHEA-S, according to age- and gender-specific DHEA-S values, can effectively rule out HPAI. However, DHEA-S alone is insufficient for the diagnosis of HPAI, and its low values should be considered in addition to other adrenal function tests. Serum DHEA-S is utilized as a screening tool for the diagnosis of HPAI and is recommended for this purpose. It is important to note that access to a short cosyntropin test is not always available, and insulin stress testing poses a risk in our region [4, 5, 16].
In a study conducted by Hahner et al., the ratio of male to female participants with AI was 113:77, with a median age of 59 years [17]. The predominance of female HPAI can be attributed to more frequent use of corticosteroids, which is somewhat unclear.
Our study found that the best results were associated with serum cortisol levels from 9 to 11 a.m., with a morning serum cortisol level <5.31 μg/dL consistent with a diagnosis of HPAI. Other researchers suggest that a serum cortisol level ≤5 μg/dL confirms the presence of HPAI [18].
In children, some experts suggest a normal, unstimulated serum cortisol level of 13.8 μg/dL. They recommend dynamic stimulation testing for those with morning cortisol levels ranging from 3.9-13.8 μg/dL [19]. DHEA-S cannot effectively distinguish primary AI from secondary AI, and low DHEA-S levels have also been observed in post-traumatic stress disorder and depressive symptoms [20].
Plasma ACTH showed the worst efficacy in this study. This result has been confirmed previously, while its use in the diagnosis of primary AI has been proven. This can be explained by the fact that impaired cortisol in HPAI is due to an ACTH-independent mechanism, e.g., decreased secretion and metabolism of cortisol by the liver and kidneys. This led to the term "relative insufficiency of the hypothalamic-pituitary-adrenal axis" [13, 21-24]. These mechanisms can increase cortisol levels during stress and be life-saving, but stress lasting more than a week affects the integrity and function of the adrenal cortex [25].
Additionally, the diminished response to exogenous ACTH may indicate inadequate ACTH signaling in the adrenal cortex. This can influence the outcome of dynamic tests to diagnose HPAI. Consequently, the short cosyntropin test has low sensitivity with a wide range of values (57-79%). However, if a short cosyntropin test is normal, it confirms the good functioning of the HPA axis [13, 26].
This study examined the use of a combination test with two or more parameters to predict HPAI and found that morning cortisol and DHEA-S provided the best predictive value. Many endocrinologists recommend this approach. A three-test panel, which includes serum cortisol, serum DHEA-S, and plasma ACTH, will offer the best specificity, albeit very low sensitivity. Mansour et al. [14] reported the prevalence of steroid use was 2.6%, which, according to the World Health Organization classification, means that the condition is rare. In this case, it is essential to have a test that can confirm the presence of the disease to avoid treatment intervention and unnecessary anxiety. On the one hand, the probability of a positive test result was 64.8%, which strongly confirms the presence of HPAI. On the other hand, the probability of a negative test result was approximately 0.83%, which rules out HPAI in approximately 99% of cases, but missed cases still exist.
Conversely, the likelihood of a negative morning cortisol test for HPAI has decreased to about 0.36%. This contrasts with the report by Mansuor et al., which helps rule out AI and makes it suitable as a screening tool.
A potential practical application of these study results is that DHEA-S could be used as a diagnostic tool for HPAI in the afternoon, since DHEA-S levels do not have circadian rhythms due to its long half-life. Since most cases of HPAI are admitted to emergency departments or hospitals in the afternoon, when conducting the short cosyntropin stimulation test is not feasible, serum cortisol and plasma ACTH levels become unreliable [10, 19, 20, 25-27].
Conclusion
Diagnosing AI is important. Measuring morning cortisol levels is a simple and convenient tool for detecting HPAI; however, DHEA-S is an alternative during the day due to its longer half-life. Using a combination of laboratory tests (cortisol + DHEA-S panel or the most effective cortisol + DHEA-S + ACTH panel) is a powerful tool for confirming HPAI.
Limitations
One of the limitations of our study was the small number of men in the sample, as well as the limited number of participants using steroids in the course of their treatment, which made it difficult to conduct a subgroup analysis.
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical approval
All study participants provided verbal informed consent, and the Ethics Committee of Basra College of Medicine approved the study protocol.
- Nicolaides NC, Charmandari E, Chrousos GP, Kino T. Circadian endocrine rhythms: The hypothalamic-pituitary-adrenal axis and its actions. Ann N Y Acad Sci 2014; 1318(1): 71-80. https://doi.org/10.1111/nyas.12464.
- Charmandari E, Kino T, Chrousos G. Glucocorticoids. In: Yaffe SJ, Aranda JV. Neonatal and Pediatric Pharmacology: Therapeutic Principles in Practice. 4th Ed. Philadelphia: Lippincott Williams and Wilkins. 2010: 760-772.
- Schmidt IL, Lahner H, Mann K, Petersenn S. Diagnosis of adrenal insufficiency: Evaluation of the corticotropin-releasing hormone test and basal serum cortisol in comparison to the insulin tolerance test in patients with hypothalamic-pituitary-adrenal disease. J Clin Endocrinol Metab 2003; 88(9): 4193-4198. https://doi.org/10.1210/jc.2002-021897.
- Al-Aridi R, Abdelmannan D, Arafah BM. Biochemical diagnosis of adrenal insufficiency: The added value of dehydroepiandrosterone sulfate measurements. Endocr Pract 2011; 17(2): 261-270. https://doi.org/10.4158/EP10262.RA.
- Nasrallah MP, Arafah BM. The value of dehydroepiandrosterone sulfate measurements in the assessment of adrenal function. J Clin Endocrinol Metab 2003; 88(11): 5293-5298. https://doi.org/10.1210/jc.2003-030449.
- Arafah BM. Hypothalamic pituitary adrenal function during critical illness: Limitations of current assessment methods. J Clin Endocrinol Metab 2006; 91(10): 3725-3745. https://doi.org/10.1210/jc.2006-0674.
- Sayyed Kassem L, El Sibai K, Chaiban J, Abdelmannan D, Arafah BM. Measurements of serum DHEA and DHEA sulphate levels improve the accuracy of the low-dose cosyntropin test in the diagnosis of central adrenal insufficiency. J Clin Endocrinol Metab 2012; 97(10): 3655-3662. https://doi.org/10.1210/jc.2012-1806.
- Arafah BM, Kailani SH, Nekl KE, Gold RS, Selman WR. Immediate recovery of pituitary function after transsphenoidal resection of pituitary macroadenomas. J Clin Endocrinol Metab 1994; 79(2): 348-354. https://doi.org/10.1210/jcem.79.2.8045946.
- Kazlauskaite R, Evans AT, Villabona CV, Abdu TA, Ambrosi B, Atkinson AB, et al. Corticotropin tests for hypothalamic-pituitary-adrenal insufficiency: A meta-analysis. J Clin Endocrinol Metab 2008; 93(11): 4245-4253. https://doi.org/10.1210/jc.2008-0710.
- Dorin RI, Qualls CR, Crapo LM. Diagnosis of adrenal insufficiency. Ann Intern Med 2003; 139(3): 194-204. https://doi.org/10.7326/0003-4819-139-3-200308050-00009.
- Mayo Clinic Laboratories. Test Id: DHES1. Dehydroepiandrosterone Sulfate, Serum. https://www.mayocliniclabs.com/test-catalog/overview/113595.
- Oelkers W. Adrenal insufficiency. N Engl J Med 1996; 335(16): 1206-1212. https://doi.org/10.1056/NEJM199610173351607.
- Broersen LH, Pereira AM, Jørgensen JOL, Dekkers OM. Adrenal insufficiency in corticosteroids use: Systematic review and meta-analysis. J Clin Endocrinol Metab 2015; 100(6): 2171-2180. https://doi.org/10.1210/jc.2015-1218.
- Mansour AA, Odaa AH, Wanoose HL. Corticosteroid nonprescription use: a cross-sectional hospital-based study in Basrah. Med Princ Pract 2010; 19(3): 182-187. https://doi.org/10.1159/000285283.
- Crowley R, Argese N, Tomlinson J, Stewart P. Central hypoadrenalism. J Clin Endocrinol Metab 2014; 99(11): 4027-4036. https://doi.org/10.1210/jc.2014-2476.
- Jones S, Trainer P, Perry L, Wass J, Besser G, Grossman A. An audit of the insulin tolerance test in adult subjects in an acute investigation unit over one year. Clin Endocrinol (Oxf) 1994; 41(1): 123-128. https://doi.org/10.1111/j.1365-2265.1994.tb03793.x.
- Hahner S, Loeffler M, Bleicken B, Drechsler C, Milovanovic D, Fassnacht M, et al. Epidemiology of adrenal crisis in chronic adrenal insufficiency: The need for new prevention strategies. Eur J Endocrinol 2010; 162(3): 597-602. https://doi.org/10.1530/EJE-09-0884.
- Dorsey MJ, Cohen LE, Phipatanakul W, Denufrio D, Schneider LC. Assessment of adrenal suppression in children with asthma treated with inhaled corticosteroids: Use of dehydroepiandrosterone sulfate as a screening test. Ann Allergy Asthma Immunol 2006; 97(2): 182-186. https://doi.org/10.1016/S1081-1206(10)60010-5.
- Maguire AM, Biesheuvel CJ, Ambler GR, Moore B, McLean M, Cowell CT. Evaluation of adrenal function using the human corticotrophin‐releasing hormone test, low dose Synacthen test and 9am cortisol level in children and adolescents with central adrenal insufficiency. Clin Endocrinol (Oxf) 2008; 68(5): 683-691. https://doi.org/10.1111/j.1365-2265.2007.03100.x.
- Usta MB, Tuncel OK, Akbas S, Aydin B, Say GN. Decreased dehydroepiandrosterone sulphate levels in adolescents with post-traumatic stress disorder after single sexual trauma. Nord J Psychiatry 2016; 70(2): 116-120. https://doi.org/10.3109/08039488.2015.1056752.
- Rothwell P, Udwadia Z, Lawler P. Cortisol response to corticotropin and survival in septic shock. Lancet 1991; 337(8741): 582-583. https://doi.org/10.1016/0140-6736(91)91641-7.
- Annane D, Sébille V, Troché G, Raphaël JC, Gajdos P, Bellissant E. A 3-level prognostic classification in septic shock based on cortisol levels and cortisol response to corticotropin. JAMA 2000; 283(8): 1038-1045. https://doi.org/10.1001/jama.283.8.1038.
- Annane D, Sebille V, Charpentier C. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. ACC Current Journal Review 2003; 12(1): 14-15. https://doi.org/10.1016/S1062-1458(02)00997-2.
- Cooper MS, Stewart PM. Corticosteroid insufficiency in acutely ill patients. N Engl J Med 2003; 348(8): 727-734. https://doi.org/10.1056/NEJMra020529.
- Boonen E, Bornstein SR, Van den Berghe G. New insights into the controversy of adrenal function during critical illness. Lancet Diabetes Endocrinol 2015; 3(10): 805-815. https://doi.org/10.1016/S2213-8587(15)00224-7.
- Ferrante E, Morelli V, Giavoli C, Mantovani G, Verrua E, Sala E, et al. Is the 250 µg ACTH test a useful tool for the diagnosis of central hypoadrenalism in adult patients with pituitary disorders? Hormones (Athens) 2012; 11(4): 428-435. https://doi.org/10.14310/horm.2002.1374.
- Yamaji T, Ishibashi M, Takaku F, Itabashi A, Katayama S, Ishii J. Serum dehydroepiandrosterone sulfate concentrations in secondary adrenal insufficiency. J Clin Endocrinol Metab 1987; 65(3): 448-451. https://doi.org/10.1210/jcem-65-3-448.
Received 4 June 2025, Revised 19 November 2025, Accepted 5 March 2026
© 2025, Russian Open Medical Journal
Correspondence to Alhamza, Ali Hussein Ali. Email: ali.alhamza@fdemc.iq.