Introduction
Shared decision-making (SDM) is a healthcare communication model that emphasizes collaboration between patients and health care providers to ensure that medical decisions align with patient values and preferences. Unlike traditional paternalistic models where physicians dominate decision-making, SDM prioritizes patient autonomy while leveraging expertise of a health care provider [1]. This approach is increasingly recommended as the gold standard in healthcare communication by prominent organizations such as the American College of Obstetricians and Gynecologists (ACOG) and the Association of American Physicians (AAP) [2, 3]. SDM is particularly relevant for preference-driven decisions, where multiple medically appropriate options exist and the optimal choice depends on the patient’s assessment of the relative importance of potential outcomes [4]. In family planning counseling, SDM has significant potential to improve decision-making about contraceptive methods. The choice of contraception is inherently a preference-driven decision, as most methods are medically appropriate for many people. Women often approach contraceptive choices differently, considering factors such as effectiveness, duration, or potential side effects, such as changes in their menstrual cycle [5, 6]. SDM model implementation enables physicians and patients to engage in a two-way dialogue in which the patient shares her values, preferences, and reproductive goals, while the physician provides evidence-based medical knowledge about contraceptive options. This collaboration enables patients to make informed and personalized choices [1].
Evidence underscores the importance of SDM in family planning. Women who participated in SDM during contraceptive counseling reported greater satisfaction with both the counseling process and the contraceptive method they chose compared with those who experienced decisions made by a physician or patient. SDM fosters a therapeutic partnership that recognizes the experiences of both parties, thereby leading to improved counseling quality, higher user satisfaction, and more effective contraceptive decisions [7].
To date, most publications have focused on describing SDM concepts, evaluating individual decision aids, or examining SDM processes, rather than systematically mapping SDM implementation factors at the physician (provider), patient, and environmental levels in family planning counseling. Family planning counseling often involves multilevel challenges, including barriers to communication with the provider, patient preferences, and systemic or environmental constraints [8]. These issues can hinder contraceptive use and reduce the effectiveness of counseling. However, existing research underexamined these aspects, leaving a critical gap in the literature. This review is the first to synthesize and classify these factors using an implementation-focused approach, integrating data from both provider and client perspectives. It thus expands on previous research on SDM in contraceptive counseling. It provides a structured framework that can serve as the basis for targeted interventions, training, and policies aimed at strengthening SDM in family planning services.
Material and Methods
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines [9].
Eligibility criteria
This review included couples of reproductive age, women and men, who were participants or potential participants in family planning programs. Health care providers involved in contraceptive counseling, including midwives, nurses, general practitioners, obstetricians and gynecologists, and family planning counselors, were also included. The study focused on the use of SDM in family planning or contraceptive counseling, with a focus on factors influencing its implementation. These factors were categorized as patient-related (e.g., preferences and motivations), provider-related (e.g., communication and interaction), and environmental (e.g., cultural norms, system policies, and regulations). The study focused on the effectiveness of SDM in improving the quality of contraceptive decisions, user satisfaction, and overall experience of counseling.
The review included studies that investigated factors influencing the implementation of SDM in family planning or contraceptive counseling, examined the use of SDM to improve decision-making and user satisfaction, or provided empirical data. Original studies using quantitative, qualitative, and mixed methods were included. Only articles published in English or Indonesian were selected; official translations were allowed. Exclusion criteria were as follows: studies unrelated to SDM in family planning, studies focusing solely on contraceptive methods without decision-making aspects, and studies focusing on nonreproductive populations or irrelevant health settings. Editorials, commentaries, non-systematic reviews, and unavailable full-text articles were also excluded.
Search algorithm
For each database, controlled vocabulary and free-text terms were combined using Boolean operators. In PubMed, the primary search string was: (“shared decision making” OR “decision making”) AND (“family planning services” OR “family planning counseling” OR contraception) AND (factor* OR determinant* OR barrier* OR facilitator* OR outcome* OR satisfaction). In addition, the reference lists of key articles on SDM and contraceptive counseling identified in the search were reviewed to ensure that influential studies were included, such as the publication by Dehlendorf et al. on SDM in contraceptive counseling and the study by Munro et al. on factors influencing the implementation of SDM in contraceptive care. Similar combinations of terms related to SDM, family planning/contraception, and factors/determinants, limited to the title and abstract fields, were adapted for ProQuest, Cochrane CENTRAL, and ScienceDirect according to the syntax of each database. The search was initially conducted on March 15, 2024, and updated on July 1, 2024, with no date restrictions.
Data screening and extraction
Two independent reviewers screened the articles to ensure consistency and minimize bias. Disagreements on eligibility were resolved through discussion with a third reviewer. A structured data capture form included the following variables: first author and year of publication, country and study setting, study design, sample size and participant characteristics (providers and/or clients), SDM framework or intervention, description of the contraceptive or family planning counseling context, SDM methods or operationalization, and detailed provider-, patient-, and setting-related determinants identified in each study. In addition, information on SDM-related outcomes (e.g., satisfaction, decisional conflict, perceived autonomy) and key methodological notes (data collection methods, analytic approach) were recorded to support comparative analysis. In line with established review methodology, the primary goal of this study was to map the range and nature of the evidence guiding the implementation of SDM in family planning counseling, rather than to assess intervention effects. Therefore, no formal assessment of the risk of bias or quality of individual studies was conducted. However, for each study, key methodological features (study design, data collection methods, and analytical approaches) were provided to facilitate interpretation of the results.
Results
The database search yielded a total of 1,632 records that were screened and assessed for relevance according to the PRISMA flow diagram (Figure 1). After removing duplicates and applying the selection criteria, 10 studies were included in the review. These studies were selected in terms of their focus on factors influencing the implementation of SDM in family planning counseling. A summary of these studies is provided in the Table 1, while Figure 2 shows the identified factors.
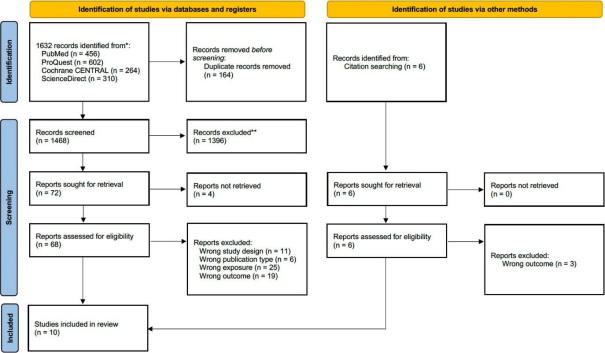
Figure 1. PRISMA flow diagram of the study selection process.
Table 1. Summary of reviewed studies
|
No. |
Study |
Study design |
Study population |
Shared decision-making (SDM) framework |
Factors influencing SDM implementation |
|
|
Provider’s perspective |
||||||
|
1. |
Munro et al. (2019) |
Qualitative study with randomized controlled trial (RCT) |
Clinical and administrative staff aged 18 years and older, employed at one of the 12 clinics participating in the experimental group, with access to email and consent to audio recording (n=29) |
Patient-centered intervention (videos and cue cards) and provider-centered intervention (decision aids and interaction training) |
FACTORS RELATED TO HEALTH CARE PROVIDERS
PATIENT-RELATED FACTORS
|
|
|
Client’s perspective |
||||||
|
2. |
Korger et al. (2021) |
Exploratory data analysis (EDA) |
Women aged 18 to 35 years who were taking oral contraceptives at the time of the study (n=217) |
Narrative, non-narrative (without personal information about experience), and control text |
FACTORS RELATED TO HEALTH CARE PROVIDERS
PATIENT-RELATED FACTORS
|
|
|
3. |
Grant et al. (2020) |
EDA (cross- sectional survey) |
The study included individuals aged 18 to 45 years, assigned female at birth, speaking English, and using or having previously used contraception (n=669) |
Anonymous web-based survey using the SURE Decisional Conflict Scale and the 9-item Shared Decision Making Questionnaire (SDM-Q-9) |
FACTORS RELATED TO HEALTH CARE PROVIDERS
PATIENT-RELATED FACTORS
|
|
|
4. |
Armuand et al. (2024) |
Phenomenological research |
Women aged 15–45 years (n=24) |
N/A |
FACTORS RELATED TO HEALTH CARE PROVIDERS
ENVIRONMENTAL FACTORS
|
|
|
5. |
Dehlendorf et al. (2010) |
Cross-sectional survey |
Women who chose progestogen-only or barrier methods of contraception after surgical abortion (n=266) |
N/A |
PATIENT-RELATED FACTORS
|
|
|
6. |
Carvajal et al. (2016) |
EDA (focus groups and semi-structured interviews) |
Hispanic women aged 15 to 24 years who were not pregnant or planning to become pregnant at the time of the interview (n=16) |
The theory of planned behavior (TPB) |
FACTORS RELATED TO HEALTH CARE PROVIDERS
ENVIRONMENTAL FACTORS
|
|
|
7. |
Meier et al. (2019) |
EDA (in-depth interviews) |
Women of reproductive age (18–45 years) residing in South Carolina who had knowledge and experience with contraception, including different types of contraceptives and patient-provider communication about contraception, and the ability to complete the interview in English or Spanish (n=38) |
N/A |
FACTORS RELATED TO HEALTH CARE PROVIDERS
PATIENT-RELATED FACTORS
ENVIRONMENTAL FACTORS
|
|
|
Shared perspective of providers and clients |
||||||
|
8. |
Johnson et al. (2010) |
EDA (pre-post design without a control group) |
Health care providers and patients in Indonesia (n=12 and 96, respectively), Mexico (n=13 and 83, respectively), and Nicaragua (n=59 and 426, respectively) |
The WHO Decision-Making Tool for Family Planning Clients and Providers |
FACTORS RELATED TO HEALTH CARE PROVIDERS
|
|
|
9. |
Dehlendorf et al. (2017) |
EDA (cross- sectional survey) |
Women recruited during contraceptive counseling at six clinics in the San Francisco Bay Area (n=345) and their health care providers (n=38) |
N/A |
PATIENT-RELATED FACTORS
|
|
|
10. |
Dehlendorf et al. (2019) |
RCT |
Inclusion criteria for health care providers: providing family planning counseling and planning services for six months (n=28). Inclusion criteria for patients: age 15 to 45 years; willingness to discuss starting or switching contraceptive methods at one of the participating clinics; having sexual intercourse with men; and ability to speak, read, and understand English or Spanish (n=758). |
My Birth Control tool group and the control group |
FACTORS RELATED TO HEALTH CARE PROVIDERS
|
|
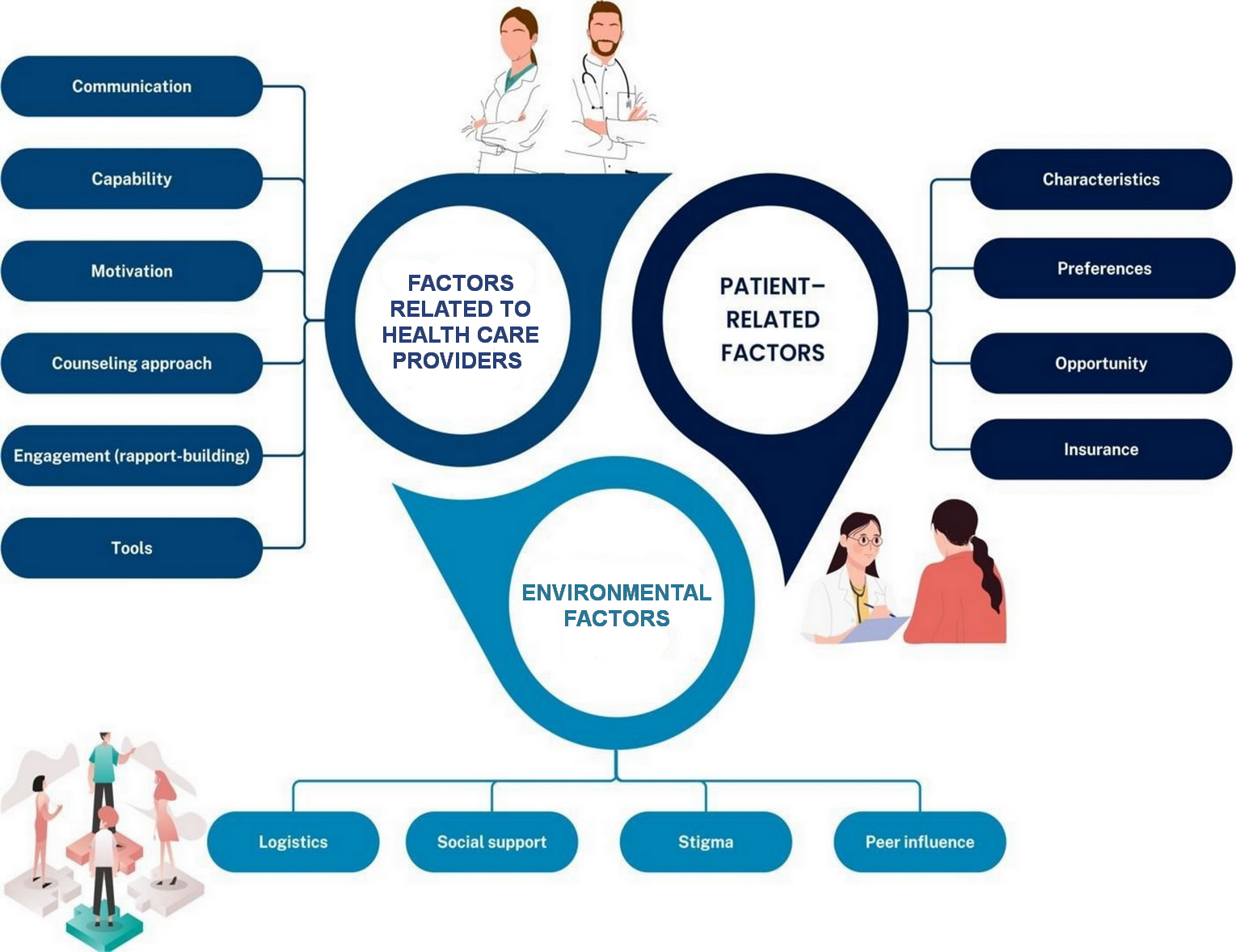
Figure 2. Factors influencing the implementation of the principle of shared decision-making in family planning counseling.
Provider-related factors
Factors influencing the implementation of SDM in family planning counseling include provider-related factors such as competence, motivation, opportunity, communication, trustworthiness, counseling approaches, engagement, tools, and preferences.
As noted by Munro et al., competence includes the knowledge, skills, memory, and behavioral regulation necessary for effective counseling. Providers must have the ability to understand patients’ needs and provide information that supports decision-making. Motivation includes professional roles, outcome beliefs, and reinforcement mechanisms such as incentives that shape provider engagement in SDM. Opportunities, influenced by social and organizational contexts, reflect the role of environmental factors, resource availability, and cultural dynamics in facilitating or hindering SDM [10].
In the included studies, several specific communication behaviors emerged as particularly important for effective SDM in family planning counseling. For example, active listening and inviting patients to express their concerns, preferences, and previous experiences with contraception were consistently associated with higher satisfaction and a stronger sense of partnership [10]. Korger et al. [11] found that participants exposed to decision-making strategies or narratives felt better prepared and more satisfied with their decisions, although the differences between narrative and non-narrative approaches were not statistically significant. Effective communication involves thorough and mutually understandable exchange of information, as noted by Carvajal et al., who emphasized that strong physician-patient relationships are built on trust and clear discussion of thoughts, preferences, and concerns. This includes discussing the risks, benefits, side effects, and effectiveness of contraceptive methods [12]. Meier et al. also emphasized the critical role of communication in ensuring that patients are adequately informed, enabling them to make informed decisions [13].
The trustworthiness of health care providers significantly influences the implementation of SDM. Armuand et al. identified empathy, openness, and commitment as important qualities for building trust [14]. Counseling approaches that emphasize SDM, as noted by Grant et al., were more effective when physicians did not recommend specific methods, allowing patients to actively participate in the decision-making process [15]. Engagement, including rapport-building and person-centered counseling, facilitates SDM via facilitating interactive processes that prioritize patient preferences and long-term outcomes [14]. Avoiding assumptions based on ethnicity or language, as noted by Carvajal et al., is crucial to ensuring personalized counseling and respect for individual needs [12]. Meier et al. also emphasized the importance of strong relationships with health care providers to enhance patient comfort and ensure informed discussions [13].
Decision-making tools also play a key role in supporting the implementation of SDM. Johnson et al. found that the WHO Decision-Making Tool for Family Planning Clients and Providers improved counseling practices through the use of the Vroom-Yetton normative decision model [16]. Similarly, Dehlendorf et al. demonstrated that tools such as My Birth Control tool increased patients’ confidence and knowledge, thereby leading to more informed decisions [17]. These factors collectively highlight the need to consider provider-related factors and integrate tools to improve SDM in family planning counseling.
Patient-related factors
Patient-related aspects also play a significant role in shaping the implementation of SDM in family planning counseling. Patient characteristics play a central role in shaping the interactions between clients and providers. Grant et al. noted that 33.8% of participants reported being discouraged from using certain contraceptive methods, with African Americans, married or cohabiting individuals, and parous women who had given birth more likely to experience such dissuade [15]. Dehlendorf et al. found that patients with prior experiences with their physicians were less likely to experience provider-initiated decision-making and more likely to engage in SDM. Furthermore, younger patients were more likely to perceive their physicians as having certain preferences, suggesting that age and previous relationships with them may influence the degree of SDM [7].
Preferences and motivations also influence SDM in family planning. Korger et al. identified the following factors that patients consider when choosing contraceptive methods: the method effectiveness, well-being during use, familiarity with the method, tolerability, control over effectiveness, and minimization of use errors [11]. Grant et al. also emphasized the importance of effectiveness, accessibility/affordability, and low risk of side effects [15], while Meer et al. added that lifestyle compatibility, cost, and consistency are critical factors. These preferences highlight the need for counseling that aligns with individual motivations and priorities [13].
Insurance coverage further influences client decision autonomy. Dehlendorf et al. reported that individuals with Medicaid insurance were less likely to desire autonomous decision-making vs. those with private insurance or self-pay [18]. These client-related factors (patient characteristics, preferences, and insurance) reflect the challenges of implementing SDM in family planning counseling and the need to adapt approaches to meet the diverse needs of clients.
Environmental factors
Environmental factors significantly influence the implementation of the SDM model in family planning counseling, affecting both the logistical and social dynamics associated with contraceptive use. Logistics, as discussed by Armuand et al., include providing adequate time for discussions, creating a comfortable environment, and ensuring services are easily accessible [14]. These factors help create a supportive environment, encouraging patients to engage in meaningful discussions and make informed decisions.
Social support also plays a crucial role in contraceptive decision-making. Carvajal et al. noted that support from family, friends, and school served as positive motivators for contraceptive use, emphasizing the importance of a patient’s social network in shaping their choice [12]. Similarly, peer influence was noted by Meier et al., who pointed out that friends (particularly, other women) often serve as key sources of information and significantly influence acceptability and decisions regarding contraceptive methods [13]. Their opinions and experiences provide valuable insights that influence how participants perceive and choose contraceptive options.
Stigma surrounding contraceptive use is a complex issue. Meier et al. noted that although many participants viewed contraception as a way to empower women, allowing them to exercise greater control over their lives, there was also a sense of shame associated with its use [13]. However, religious ideologies and societal norms were rarely mentioned as significant barriers, suggesting that stigma may vary depending on individual and contextual factors. Environmental factors require counseling approaches that aim to remove barriers, promote support, and reduce stigma to improve SDM adoption.
Discussion
SDM in family planning counseling depends on factors related to health care providers, patients, and the environment. Health care provider competence, including knowledge, skills, motivation, and the use of decision aids, is essential. Communication skills and rapport-building strengthen the process, while counseling methods supported by aids such as the WHO Decision-Making Tool or My Birth Control tool enhance engagement. Patient-related factors, such as age, relationship with the health care provider, preferences, cost, and lifestyle compatibility, influence participation, while insurance and access to services influence decision autonomy. Environmental factors, including logistics, social support, and stigma, also influence SDM implementation.
The results also indicate that provider-related, patient-related, and environmental factors that determine SDM interact dynamically rather than acting in isolation [10, 12]. Time constraints and organizational pressure from healthcare providers, described as logistical barriers to contraceptive counseling, may push physicians toward a more directive style. This, in turn, limits opportunities for young or socially disadvantaged patients to express their preferences and ask questions. When healthcare providers have strong communication skills and use structured decision support aids, such as the WHO Decision-Making Tool or My Birth Control tool, these strategies can partially offset patient-level barriers (low health literacy, previous negative experiences, or uncertainty) by organizing information and encouraging clarification of values. At the same time, social stigma and peer norms regarding contraception may discourage patients from disclosing their concerns and make health care providers more cautious about discussing sensitive topics, reinforcing cycles of superficial or provider-driven decision-making, despite the stated use of SDM. Recognition of these inter-level interactions supports the need for multicomponent interventions that simultaneously strengthen the capacity and motivation of health care providers, expand patient opportunities for participation, and change organizational conditions to ensure sufficient time and safety for genuine dialogue [10].
From the health care provider’s perspective, capacity, communication skills, and the use of decision support aids act as central levers for implementing SDM, while patient-related and environmental factors determine how these levers are manifested in practice. Establishing trust and rapport through clear communication is crucial for patient engagement. For example, studies by Johnson et al. and Dehlendorf et al. demonstrated that provider-focused tools significantly improved SDM outcomes by improving counseling practices and increasing patient confidence [16,17].
From the client’s perspective, autonomy, comfort, and personalized information are central elements of effective SDM. Patients value understanding their options in a judgment-free environment, and their preferences (shaped by lifestyle, cost, and effectiveness) guide their choices. Dehlendorf et al. suggested that younger patients or those who had negative experiences with providers were more likely to perceive a lack of SDM [7].
The implementation of SDM varies by region and cultural context. In countries such as Indonesia, Mexico, and Nicaragua, as shown in a study by Johnson et al., decision-making tools played a significant role in improving SDM. These regions often face logistical barriers, including limited resources and accessibility, making structured tools particularly effective [16]. In contrast, studies conducted in the United States, such as that by Meyer et al., focus more on individual preferences, social norms, and stigma. For example, although contraception was viewed as a means of empowering women, feelings of shame associated with its use were widespread [13]. However, religious ideologies and social norms were rarely mentioned as significant barriers in the United States, in contrast to other countries where religion may play a more central role in shaping contraceptive decisions [19, 20].
The observation that some patients, particularly those with Medicaid or in certain clinical settings, report less desire to make autonomous decisions highlights how power dynamics and structural inequalities shape the experience and feasibility of SDM in family planning [16]. In settings where women have limited prior positive experiences with healthcare, face language or cultural barriers, or occupy marginalized socioeconomic positions, yielding to the judgement of physicians may reflect limited choice rather than a genuine desire to relinquish control and may coexist with negative attitudes toward certain practices. Differences in health literacy and access to information between regions such as Indonesia, Mexico, Nicaragua, and the United States further influence whose values are heard and considered, with decision aids and physician communication styles either reinforcing existing hierarchies or promoting a redistribution of power during consultation [13]. Recognition of such dynamics suggests that SDM interventions should be explicitly equity-focused, combining decision support tools and communication training with broader efforts to reduce economic, informational, and cultural barriers that limit patients’ ability to fully participate in contraceptive decisions.
Patient preferences when implementing SDM in family planning, particularly regarding lifestyle compatibility and cost, play a key role in contraceptive choice, highlighting the importance of individualized counseling [21]. Similar findings from broader SDM studies, such as the study by Shinkunas et al. in oncology, show that patients often prioritize options that align with personal values and lifestyle impacts. For example, breast cancer patients often choose treatment based on commitment and emotional considerations, reflecting themes observed in family planning [22].
Effective communication, trust, and rapport-building are also central to implementing SDM in family planning. Similar findings in chronic disease management, such as the Liverpool et al. study in mental health, highlight that trust and clear communication are essential for patient engagement [23]. This consistency across domains demonstrates the importance of interpersonal dynamics in SDM. The emphasis on empathy and clear communication suggests that training health care professionals in SDM should prioritize developing interpersonal skills to improve patient-provider interactions.
Systemic and environmental factors, including stigma, cultural norms, and logistical constraints, significantly influence the implementation of shared decision-making in family planning. Similar barriers are observed in broader SDM research. For instance, Shinkunas et al. reported that time constraints and cultural inconsistencies are common challenges in surgical decision-making [22]. In emergency surgical situations, insufficient time for thorough SDM reflects the logistical constraints health care professionals face when providing family planning counseling.
A notable distinction of SDM in family planning is the influence of stigma, as societal expectations and norms often shape the decision-making process. Unlike SDM in disease management, which typically emphasizes individual autonomy with minimal societal influence, contraceptive decision-making involves additional layers of complexity [22, 24, 25]. This approach should shift toward prioritizing women’s decision-making. Improving the implementation of SDM methods in family planning counseling requires targeted training to strengthen the communication and interpersonal skills of health care providers, the regular use of evidence-based decision aids, and systemic changes that reduce logistical barriers and eliminate stigma and other sociocultural constraints.
Limitations of the study
Current research on factors influencing the implementation of SDM methods in family planning counseling identified key gaps, particularly in resource-limited settings where systemic barriers and inadequate training of health care providers hinder effectiveness. The role of cultural norms and values in shaping the adoption of SDM tools remains understudied. Many studies relied on self-reported data, which carries the risk of bias, and lack longitudinal design, which would allow to assess the long-term impact of factors related to health care providers, patients, and the environment. Another important limitation is the lack of formal critical assessment of the methodological quality or risk of bias in the included studies. As a result, the presented review cannot evaluate the contribution of studies with higher and lower accuracy, and the identified determinants should be interpreted as hypothesis-generating rather than as providing definitive causal inferences. Furthermore, our search algorithm may have excluded relevant studies due to database or search term limitations, potentially missing important literature. Language limitations further narrowed the scope of the study. The heterogeneity of the included studies in terms of methodologies, settings, and measured outcomes poses challenges in generalizing results and drawing definitive conclusions. These limitations highlight the need for comprehensive future reviews to address these gaps and provide a deeper understanding of the factors influencing the implementation of SDM.
Key points:
- The implementation of SDM in family planning counseling is determined by the interaction of provider, patient, and environmental factors, rather than by individual factors;
- Provider communication skills, empathy, and the use of structured decision aids (e.g., the WHO Decision-Making Tool, My Birth Control tool) are central to supporting informed and value-consistent contraceptive choices;
- Patient characteristics, preferences, previous health care experiences, and insurance or financial barriers influence the extent to which autonomy and participation in decision-making are feasible and desirable;
- Environmental conditions, including time constraints, logistics, social support, and contraceptive use stigma, can either facilitate or hinder effective SDM;
- Equity-focused SDM interventions should simultaneously consider provider capacity, patient empowerment, and structural barriers to ensure that SDM is realistic for women across diverse sociocultural and economic contexts.
Conclusion
This scoping review examines the factors shaping the implementation of SDM in family planning counseling, taking into account provider, patient, and environmental aspects using an implementation-focused approach. By integrating data from both health care providers and contraceptive users across diverse settings, it offers a structured framework explaining how capacity, communication, preferences, and contextual constraints interact to shape the feasibility and experience of SDM in contraceptive care.
Conflict of interest
The authors declare no conflicts of interest.
AI statement
We confirm that no AI or AI-assisted technologies were used in the preparation of this manuscript.
- Bullington BW, Sata A, Arora KS. Shared decision-making: The way forward for postpartum contraceptive counseling. Open Access J Contracept 2022; 13: 121-129. https://doi.org/10.2147/oajc.s360833.
- Menon S; Committee on Adolescence. Long-acting reversible contraception: Specific issues for adolescents. Pediatrics 2020; 146(2): e2020007252. https://doi.org/10.1542/peds.2020-007252.
- Ryan GL, Brandi K. Informed consent and shared decision making in obstetrics and gynecology. Obstet Gynecol 2021; 137(2): e1-e15. https://doi.org/10.1097/aog.0000000000004248.
- Elwyn G, Dehlendorf C, Epstein RM, Marrin K, White J, Frosch DL. Shared decision making and motivational interviewing: achieving patient-centered care across the spectrum of health care problems. Ann Fam Med 2014; 12(3): 270-275. https://doi.org/10.1370/afm.1615.
- Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (Or it takes at least two to tango). Soc Sci Med 1997; 44(5): 681-692. https://doi.org/10.1016/S0277-9536(96)00221-3.
- Lessard LN, Karasek D, Ma S, Darney P, Deardorff J, Lahiff M, et al. Contraceptive features preferred by women at high risk of unintended pregnancy. Perspect Sex Reprod Health 2012; 44(3): 194-200. https://doi.org/10.1363/4419412.
- Dehlendorf C, Grumbach K, Schmittdiel JA, Steinauer J. Shared decision making in contraceptive counseling. Contraception 2017; 95(5): 452-455. https://doi.org/10.1016/j.contraception.2016.12.010.
- Bullington BW, Arora KS. Fulfillment of desired postpartum permanent contraception: A health disparities issue. Reprod Sci 2022; 29(9): 2620-2624. https://doi.org/10.1007/s43032-022-00912-3.
- Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann Intern Med 2018; 169(7): 467-473. https://doi.org/10.7326/M18-0850.
- Munro S, Manski R, Donnelly KZ, Agusti D, Stevens G, Banach M, et al. Factors influencing implementation of shared decision making in contraceptive care: A qualitative interview study among clinical and administrative staff. Implement Sci 2019; 14(1): 95. https://doi.org/10.1186/s13012-019-0941-z.
- Korger S, Eggeling M, Cress U, Kimmerle J, Bientzle M. Decision aids to prepare patients for shared decision making: Two randomized controlled experiments on the impact of awareness of preference-sensitivity and personal motives. Health Expect 2021; 24(2): 257-268. https://doi.org/10.1111/hex.13159.
- Carvajal DN, Gioia D, Mudafort ER, Brown PB, Barnet B. How can primary care physicians best support contraceptive decision making? A qualitative study exploring the perspectives of Baltimore Latinas. Womens Health Issues 2017; 27(2): 158-166. https://doi.org/10.1016/j.whi.2016.09.015.
- Meier S, Sundstrom B, Delay C, DeMaria AL. "Nobody's Ever Told Me That:" Women's Experiences with Shared Decision-making when Accessing Contraception. Health Commun 2021; 36(2): 179-187. https://doi.org/10.1080/10410236.2019.1669271.
- Armuand G, Grandahl M, Volgsten H, Stern J. Characteristics of good contraceptive counselling – An interview study. Sex Reprod Healthc 2024; 39: 100948. https://doi.org/10.1016/j.srhc.2024.100948.
- Grant RL, Paul R, Zeal C, Madden T, Politi MC. Decisional conflict associated with clinicians discouraging particular contraceptive methods. J Eval Clin Pract 2020; 26(6): 1612-1619. https://doi.org/10.1111/jep.13364.
- Johnson SL, Kim YM, Church K. Towards client-centered counseling: development and testing of the WHO Decision-Making Tool. Patient Educ Couns 2010; 81(3): 355-361. https://doi.org/10.1016/j.pec.2010.10.011.
- Dehlendorf C, Reed R, Fitzpatrick J, Kuppermann M, Steinauer J, Kimport K. A mixed-methods study of provider perspectives on My Birth Control: a contraceptive decision support tool designed to facilitate shared decision making. Contraception 2019; 100(5): 420-423. https://doi.org/10.1016/j.contraception.2019.08.001.
- Dehlendorf C, Diedrich J, Drey E, Postone A, Steinauer J. Preferences for decision-making about contraception and general health care among reproductive age women at an abortion clinic. Patient Educ Couns 2010; 81(3): 343-348. https://doi.org/10.1016/j.pec.2010.06.021.
- Yillah RM, Bull F, Sawaneh A, Reindorf B, Turay H, Wurie HR, et al. Religious leaders' nuanced views on birth spacing and contraceptives in Sierra Leone – qualitative insights. Contracept Reprod Med 2024; 9(1): 40. https://doi.org/10.1186/s40834-024-00301-y.
- Barro A, Bado AR. Religious Leaders' Knowledge of Family Planning and Modern Contraceptive Use and Their Involvement in Family Planning Programmes in Burkina Faso: A Qualitative Study in Dori in the Sahel Region. Open Access J Contracept 2021; 12: 123-132. https://doi.org/10.2147/OAJC.S315395.
- Fonu PDD, Asravor RK, Sackey FG, Obuobisa-Darko T The power of faith: how religion shapes the decision making and choices of Ghanaian consumers – insights from a cross-sectional study. Cogent Arts Humanit 2024; 11(1): 2438489. https://doi.org/10.1080/23311983.2024.2438489.
- Shinkunas LA, Klipowicz CJ, Carlisle EM. Shared decision making in surgery: a scoping review of patient and surgeon preferences. BMC Med Inform Decis Mak 2020; 20(1): 190. https://doi.org/10.1186/s12911-020-01211-0.
- Liverpool S, Pereira B, Hayes D, Wolpert M, Edbrooke-Childs J. A scoping review and assessment of essential elements of shared decision-making of parent-involved interventions in child and adolescent mental health. Eur Child Adolesc Psychiatry 2021; 30(9): 1319-1338. https://doi.org/10.1007/s00787-020-01530-7.
- Morrison T, Foster E, Dougherty J, Barton J. Shared decision making in rheumatology: A scoping review. Semin Arthritis Rheum 2022; 56: 152041. https://doi.org/10.1016/j.semarthrit.2022.152041.
- Niburski K, Guadagno E, Mohtashami S, Poenaru D. Shared decision making in surgery: A scoping review of the literature. Health Expect 2020; 23(5): 1241-1249. https://doi.org/10.1111/hex.13105.
Received 25 September 2025, Revised 20 December 2025, Accepted 5 March 2026
© 2025, Russian Open Medical Journal
Correspondence to Syah Rini Wisdayanti. E-mail: syahrini_spog1@staff.uns.ac.id.