Introduction
Pituitary adenomas are among the most common brain tumors, accounting for approximately 14% of all primary tumors of the intracranial central nervous system. Their estimated prevalence in the general population, based on imaging and autopsy data, is approximately 17% [1, 2]. They are typically classified as microadenomas <10 mm in size and macroadenomas ≥10 mm in size.
NFPAs are benign, well-differentiated, clinically nonfunctioning pituitary adenomas originating from the anterior pituitary gland (adenohypophysis). They account for approximately 14–54% of all pituitary adenomas and are considered the second most common pituitary adenomas. They are characterized by the absence of clinical and biochemical evidence of hormone excess, although mild hyperprolactinemia may occasionally occur [3, 4].
The prevalence of NFPA ranges from 7 to 41.3 cases per 100 thousand individuals, with an incidence rate of 0.65–2.34/100,000 [3, 5].
Because NFPAs do not secrete hormones and do not cause specific clinical syndromes, their presentation can vary notably: from incidental detection during imaging studies performed for unrelated reasons to symptoms such as hypopituitarism and visual impairment caused by compression of the pituitary gland and optical apparatus of the eye [6].
For NFPAs presenting with mass-effect symptoms or hypopituitarism, transsphenoidal surgery (either alone or in combination with radiation therapy) is the recommended first-line treatment [7]. However, in asymptomatic cases, decisions regarding conservative management of NFPA, including imaging and hormonal studies, are based on the estimated risk of tumor progression and the development of new hormonal imbalances, which are influenced by the natural history of NFPA [8].
The goal of this study was to evaluate the clinical characteristics, treatment modalities, complications, and outcomes of patients with NFPA treated at the Faiha Specialized Diabetes, Endocrinology, and Metabolism Center (FDEMC) in Basra, Iraq, filling the gap in comprehensive data on NFPA from Iraq and building on a previous study from FDEMC that included a smaller cohort of patients with NFPA [10].
Material and Methods
Study design and participants
This single-center retrospective study was conducted on 202 patients at the FDEMC in Basra, southern Iraq, between January 2011 and January 2025. Eligible participants were identified by searching the FDEMC electronic database for NFPA.
Inclusion criteria
Patients were included in the study if they met the following criteria:
· NFPA diagnosed radiologically and confirmed by a normal hormonal profile or mild hyperprolactinemia without other hormone hypersecretion syndromes;
· Radiological diagnosis of pituitary adenoma by direct analysis of magnetic resonance imaging (MRI) or based on MRI reports from the reputable radiology department;
· Adequate clinical and demographic documentation in the medical record.
Exclusion criteria
Patients were excluded if they met any of the following criteria:
· Diagnosis of a functioning pituitary adenoma with hormone hypersecretion syndromes other than hyperprolactinemia, which may be due to pituitary stalk interruption;
· Incomplete medical records preventing proper data extraction;
Possibility of having more than one diagnosis documented during follow-up.
Patient selection algorithm, along with their inclusion/exclusion to/from the FDEMC database, can be viewed in Figure 1.
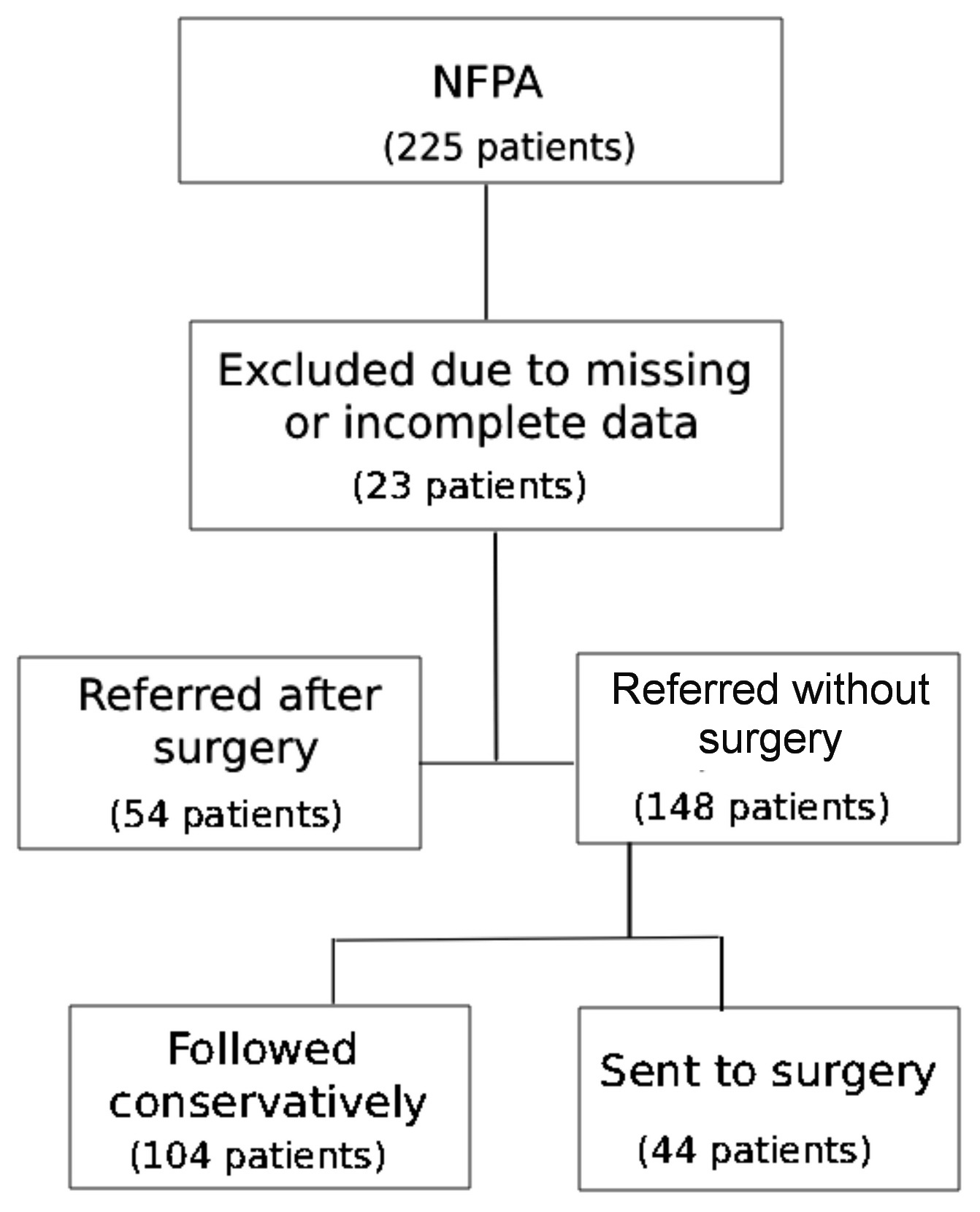
Figure 1. Patient flowchart in the non-functioning pituitary adenoma (NFPA) study.
Data collection
Data were collected retrospectively from the FDEMC electronic medical records. The following data were assessed:
· Demographic data: age, gender, and relevant medical history;
· Clinical presentation: symptoms at presentation, including visual impairment, headache, and signs of endocrine dysfunction.
· Radiology data: MRI-based tumor characteristics, including size (microadenoma vs. macroadenoma), invasiveness (e.g., cavernous sinus involvement), and optic chiasm compression;
· Treatment details: treatment type (surgery, observation, or radiation therapy), as well as any adjuvant therapies.
Definitions of clinical variables
· Hypogonadism is defined as central (hypogonadotropic) hypogonadism with reduced due to pituitary dysfunction, resulting in low sex hormone levels and low or normal gonadotropin levels;
· Hypopituitarism is specified as the partial or complete failure of the pituitary gland to produce hormones. This can affect adrenocorticotropic hormone (ACTH), thyroid-stimulating hormone (TSH), growth hormone (GH), luteinizing hormone/follicle-stimulating hormone (LH/FSH), and sometimes antidiuretic hormone (ADH), with symptoms depending on the hormone deficiency;
· Central hypothyroidism is characterized by abnormally low serum levels of free thyroxine (T4), accompanied by low, normal, or inappropriately slightly elevated TSH concentrations. This occurs due to inadequate stimulation of the structurally normal thyroid gland caused by impaired TSH secretion or action;
· Visual field defect is described as loss of part of the visual field, often due to compression of the optic chiasm. Diagnosis is made either clinically by neurological examination or by formal ophthalmological examination (perimetry);
· Galactorrhea is an inadequate milk production unrelated to childbirth or breastfeeding;
· Menstrual irregularities include infrequent, absent, or abnormal menstrual cycles;
· Infertility is defined as inability to conceive after one year of unprotected sexual intercourse.
Biochemical evaluation
A comprehensive hormonal evaluation of patients included a baseline profile and assessment of both hypersecretion and hypopituitarism [9].
Hormonal assessment of pituitary function
Basic hormonal profile:
Morning serum cortisol (at 9:00 AM), insulin-like growth factor 1 (IGF-1), prolactin, FSH, LH, estradiol (women), testosterone (men), TSH, free T4.
Evaluation for excess hormonal production:
· If IGF-1 levels are elevated, acromegaly should be assessed using GH suppression test as part of an oral glucose tolerance test;
· Rule out Cushing’s syndrome using one or more of the following methods: overnight dexamethasone suppression test or midnight salivary cortisol assay, even in asymptomatic patients;
· Hyperprolactinemia is determined biochemically by a prolactin level ≥25 μg/L.
Pituitary insufficiency assessment:
· Adrenal insufficiency is likely if morning cortisol levels are <3 mcg/dL and unlikely if they are >15 mcg/dL combined with low ACTH levels (<20);
· Central hypothyroidism is likely with low serum levels of free T4 and low, normal, or inappropriately slightly elevated TSH levels;
· Central hypogonadism is diagnosed with low estradiol levels (in women) or low testosterone levels (in men) and low/normal FSH and LH levels.
Hormonal analyses, including FSH, estradiol, prolactin, GH, TSH, free T4, total testosterone, ACTH, and cortisol, were performed using a fully automated Cobas e 411 chemiluminescence immunoassay (Roche Diagnostics, Germany). IGF-1 was measured using an enzyme-linked immunosorbent assay (ELISA).
Statistical processing of collected data
Data analysis was performed using IBM SPSS Statistics for Windows, version 27.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation, or median. Categorical variables are reported as frequencies and percentages. Comparisons between groups were performed using the Student’s t-test for continuous variables and the chi-squared test or Fisher’s exact test for categorical variables. A p-value of <0.05 was considered statistically significant.
Results
Of the 202 patients (Table 1), the mean age at presentation was 44.25±15.88 years. In patients up to 30 years of age (n=48), there was a nearly equal distribution between microadenomas (n=23 patients, 47.9%) and macroadenomas (n=25 patients, 52.1%). In the 31-50 years age group (n=80), macroadenomas were more common, occurring in 61 patients (76.3%). This trend continued in patients older than 50 years (n=74), among which 68 patients (91.9%) had macroadenomas. This age-related increase in the proportion of macroadenomas was statistically significant (p<0.001).
Table 1. Demographic data and baseline characteristics of patients (n=202) with non-functional pituitary adenoma
|
Characteristics |
Mean ± SD or N (%) |
|||
|
Patient characteristics: |
||||
|
Age (mean±SD), years |
44.25 ± 15.88 |
|||
|
|
Microadenoma, n (%) |
Macroadenoma, n (%) |
p-value |
|
|
<30 years (n=48) |
23 (47.9) |
25 (52.1) |
0.0001 |
|
|
30-50 years (n=80) |
19 (23.8) |
61 (76.2) |
||
|
>50 years (n=74) |
6 (8.1) |
68 (91.9) |
||
|
BMI (mean ± SD) |
31.03 ± 6.83 |
|||
|
Underweight (BMI <18.5) |
4 (2.0) |
|||
|
Normal weight (BMI =18.5-24.9) |
27 (13.4) |
|||
|
Overweight (BMI =25-29.9) |
66 (32.8) |
|||
|
Obese (BMI >30) |
104 (51.7) |
|||
|
Gender: |
||||
|
|
Total |
Microadenoma, n (%) |
Macroadenoma, n (%) |
p-value |
|
Female, n (%) |
120 (59.4) |
37 (30.8) |
83 (69.2) |
0.004 |
|
Male, n (%) |
82 (40.6) |
11 (13.4) |
71 (86.6) |
|
|
Adenoma characteristics: |
||||
|
Microadenoma, n (%) |
48 (23.8) |
|||
|
Macroadenoma, n (%) |
154 (76.2) |
|||
|
Incidentaloma, n (%) |
27 (13.4) |
|||
|
Chiasmal compression, n (%) |
68 (33.7) |
|||
|
Cavernous invasion, n (%) |
48 (23.8) |
|||
|
Treatment modality: |
||||
|
Conservative |
97 (48) |
|||
|
Gamma Knife and radiation therapy (RT) |
23 (11.3) |
|||
|
Gamma Knife after surgery |
17 (8.4) |
|||
|
Gamma Knife as primary treatment |
6 (3) |
|||
|
Conventional RT |
3 (1.5) |
|||
|
Surgery |
105 (52) |
|||
|
Transsphenoidal only |
88 (43.6) |
|||
|
Transcranial only |
9 (4.5) |
|||
|
Both approaches |
5 (2.5) |
|||
|
Repeat surgery |
14 (6.9) |
|||
|
Two surgeries |
10 (5) |
|||
|
Three surgeries |
3 (1.5) |
|||
|
Four surgeries |
1 (0.5) |
|||
Women constituted 120 of the 202 (59.4%) patients in the cohort. Among women, 37 of 120 (30.8%) had microadenomas, while 83 of them (69.2%) had macroadenomas. In contrast, among men, only 11 of 82 (13.4%) had microadenomas, while 71 (86.6%) were diagnosed with macroadenomas. This gender-based difference in the distribution of microadenomas and macroadenomas was statistically significant (p=0.004). The mean body-mass index (BMI) was 31.03±6.83. Of the 202 patients, 104 (51.7%) were obese, 66 (32.8%) were overweight, 27 (13.4%) had normal weight, and 4 (2.0%) were underweight. Macroadenomas were detected in 154 of 202 patients (76.2%), and in 27 of 202 (13.4%), these were incidentalomas. Chiasmal compression was observed in 68 of 202 patients (33.7%), while cavernous sinus invasion was revealed in 48 of 202 patients (23.8%).
Among the cohort (n=202), 105 patients (52%) underwent pituitary surgery, 88 (43.6%) had transsphenoidal surgery alone, 9 (4.5%) experienced transcranial surgery, and 5 patients (2.5%) underwent a combined approach. Repeat surgery was required in 14 of 202 patients (6.9%), with 10 (5%) in need of two surgeries, 3 (1.5%) undergoing three surgeries, and 1 (0.5%) requiring four interventions. Conservative treatment without surgery was used in 97 (48%) cases. Gamma Knife® surgery was employed in 23 patients (11.4%). Of 202 patients, 17 (8.4%) received postoperative treatment, while 6 (3%) received it as primary treatment and 3 patients (1.5%) required conventional radiation therapy.
The most common symptoms were headache (in 67 of 202 patients; 33.2%), isolated adrenal insufficiency (64 patients; 31.7%), visual field defects (47 patients; 23.3%), and hypopituitarism (53 patients; 26.2%) (Table 2). We compared the clinical characteristics of patients with microadenomas (n=48) and macroadenomas (n=154). Headache was statistically significantly (p=0.038) more common in macroadenomas (in 57 of 154 patients; 37.0%) vs. microadenomas (in 10 of 48 patients; 20.8%). Visual field defects were significantly more common among patients with macroadenomas (n=46; 29.9%) compared to microadenomas (n=1; 2.1%) (p<0.001). Similarly, hypopituitarism was observed in 51 (33.1%) patients with macroadenomas vs. 2 (4.2%) patients with microadenomas (p<0.001), and isolated adrenal insufficiency was significantly more common in the macroadenoma group (n=62; 40.3%) vs. 2 (4.2%) in the microadenoma group. In contrast, incidentalomas were more frequently detected in patients with microadenomas (n=13; 27.1%) than in the macroadenoma group (n=14; 9.1%) (p=0.001). We revealed no statistically significant differences between the two groups in terms of galactorrhea (p=0.066), isolated hypogonadism (p=0.105), isolated hypothyroidism (p=0.204), menstrual irregularities in women (p=0.354), and infertility (p=0.675).
Table 2. Clinical signs and symptoms depending on adenoma size in patients with non-functional pituitary adenoma (n=202)
|
Clinical characteristics |
Microadenoma Σ=48 patients, N (%) |
Macroadenoma Σ=154 patients, N (%) |
Total N (%) |
p-value |
|
Headache |
10 (20.8%) |
57 (37.0%) |
67 (33.2%) |
0.038 |
|
Visual field defect |
1 (2.1%) |
46 (29.9%) |
47 (23.3%) |
0.0001 |
|
Hypopituitarism |
2 (4.2%) |
51 (33.1%) |
53 (26.2%) |
0.0001 |
|
Galactorrhea (in women) |
9 (18.8%) |
14 (9.1%) |
23 (11.4%) |
0.066 |
|
Incidentaloma |
13 (27.1%) |
14 (9.1%) |
27 (13.4%) |
0.001 |
|
Central hypogonadism |
5 (10.4%) |
32 (20.8%) |
37 (18.3%) |
0.105 |
|
Central hypothyroidism |
4 (8.3%) |
24 (15.6%) |
28 (13.9%) |
0.204 |
|
Central adrenal insufficiency |
2 (4.2%) |
62 (40.3%) |
64 (31.7%) |
0.0001 |
|
Menstrual irregularities (in women) |
12 (25%) |
29 (18%) |
41 (20.3%) |
0.354 |
|
Infertility |
5 (10.4%) |
13 (8.4%) |
18 (8.9%) |
0.675 |
Clinical characteristics of patients who underwent surgery (n=97) vs. those who received conservative treatment (n=105) were also compared (Table 3). Visual field defects were statistically significantly more common among patients requiring surgery vs. those observed clinically: 34 of 97 (35.1%) vs. 13 of 105 (12.4%) (p=0.001). Similarly, hypopituitarism was observed in 38 (39.2%) surgical patients compared to 15 (14.3%) patients treated conservatively (p=0.001), and isolated adrenal insufficiency was observed in 43 (44.3%) of surgical patients vs. 21 (20%) patients treated conservatively (p=0.001). In contrast, incidentalomas were more frequently detected among non-operated patients: 21/105 (20.0%) vs. 6/97 (6.2%), p=0.004. No significant differences were revealed between the groups of patients who underwent surgeries vs. those who did not in the following indicators: headache (p=0.398), galactorrhea (p=0.825), isolated hypogonadism (p=0.780), isolated hypothyroidism (p=0.319), menstrual irregularities (p=0.913), and infertility (p=0.623).
Table 3. Clinical symptoms depending on surgical status in patients with non-functional pituitary adenoma (n=202)
|
Clinical characteristics |
Operated Total of 97 patients N (%) |
Not operated Total of 105 patients N (%) |
Total N (%) |
p-value |
|
Headache |
35 (36.1%) |
32 (30.5%) |
67 (33.2%) |
0.398 |
|
Visual field defect |
34 (35.1%) |
13 (12.4%) |
47 (23.3%) |
0.001 |
|
Hypopituitarism |
38 (39.2%) |
15 (14.3%) |
53 (26.2%) |
0.001 |
|
Galactorrhea (in women) |
12 (12.4%) |
11 (10.5%) |
23 (11.4%) |
0.825 |
|
Incidentaloma |
6 (6.2%) |
21 (20%) |
27 (13.4%) |
0.004 |
|
Central hypogonadism |
17 (17.5%) |
20 (19%) |
37 (18.3%) |
0.78 |
|
Central hypothyroidism |
11 (11.3%) |
17 (16.2%) |
28 (13.9%) |
0.319 |
|
Central adrenal insufficiency |
43 (44.3%) |
21 (20%) |
64 (31.7%) |
0.001 |
|
Menstrual irregularities (in women) |
20 (20.6%) |
21 (20%) |
41 (20.3%) |
0.913 |
|
Infertility |
10 (10.3%) |
8 (7.6%) |
18 (8.9%) |
0.623 |
Prolactin levels were available for 142 of 202 (70.3%) patients in the cohort, of whom 38 had microadenoma and 104 had macroadenoma. Among these 142 patients, hyperprolactinemia (serum prolactin level ≥25 ng/mL) was detected in 63 patients (44.4%). Hyperprolactinemia was established in 16 of 38 patients with microadenomas (42.1%) and 47 of 104 patients with macroadenomas (45.2%). No statistically significant association was found between adenoma size (micro vs. macro) and the presence of hyperprolactinemia. The mean prolactin level was 33.35±31.7 ng/mL in microadenomas and 34.43±29.88 ng/mL in macroadenomas (p=0.856) (Table 4).
Table 4. Prolactin levels and their distribution
|
Adenoma type |
Mean |
Median |
SD |
Hyperprolactinemia n (%) |
p-value |
|
Microadenoma |
33.35 |
20.28 |
31.7 |
16 (42.1%) |
0.849 |
|
Macroadenoma |
34.43 |
22.05 |
29.88 |
47 (45.2%) |
The stacked histogram below illustrates serum prolactin levels (x-axis, ng/mL) for two categories of pituitary adenoma:
• Microadenoma (<10 mm; blue, n=38): mean =33.3 ng/mL, standard deviation =31.7 ng/mL
• Macroadenoma (≥10 mm; teal, n=104): mean =34.4 ng/mL, standard deviation =29.8 ng/mL
The distribution is right-skewed, with most values below 40 ng/mL, and the long tail extending to approximately 120 ng/mL. Despite the larger sample size of macroadenomas, both groups exhibit virtually identical central tendencies and variability, indicating that tumor size did not significantly influence baseline prolactin levels in this cohort. Elevated prolactin levels (>60 ng/mL) are disproportionately frequent in macroadenoma cases. Microadenomas are predominantly found in the lower tail of a high-range population, and extreme outliers are almost exclusively associated with macroadenomas (Figure 2).
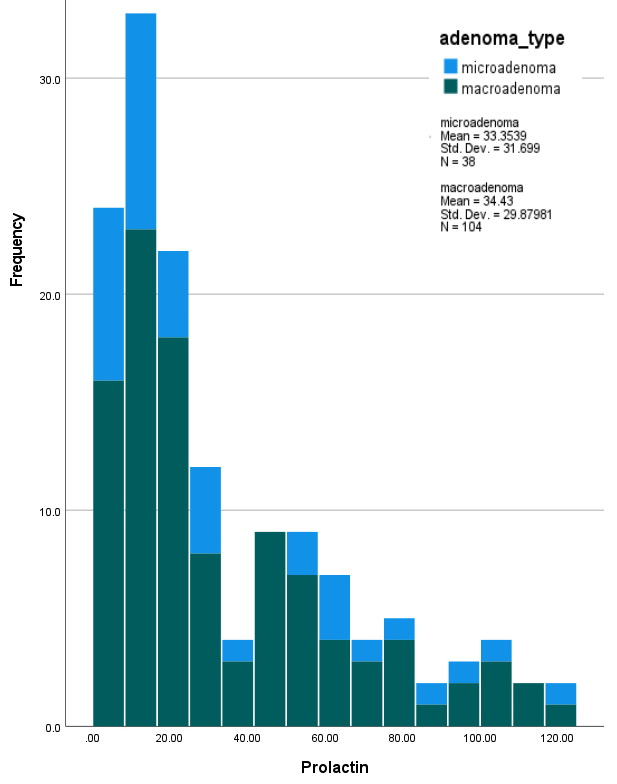
Figure 2. Histogram of prolactin distribution by adenoma type.
in 13 (6.4%) patients, cranial nerve palsy (hemianopia) in 3% of patients, cerebrospinal fluid (CSF) rhinorrhea in 3 (1.5%) patients, meningitis in 1 patient (0.5%), and apoplexy in 10 (5%) patients. Permanent blindness was observed in 7 (3.5%) patients. Residual tumor was detected postoperatively in 48 (23.8%) patients (Table 5).
Table 5. Complications and surgical outcomes
|
Complication/Outcome |
N (%) |
|
Cranial nerve palsy (hemianopia) |
6 (3%) |
|
Secondary empty sella |
38 (18.8%) |
|
Cerebrospinal fluid rhinorrhea |
3 (1.5%) |
|
Meningitis |
1 (0.5%) |
|
Arginine vasopressin deficiency |
13 (6.4%) |
|
Blindness |
7 (3.5%) |
|
Residual tumor after surgery |
48 (23.8) |
|
Apoplexy |
10 (5%) |
Discussion
A previous FDEMC study by Mansour et al. in 2018 included 49 patients with NFPA, but this study expands the cohort to 202 patients, providing a more comprehensive analysis of NFPA in Basra [10]. To our knowledge, studies of NFPA in the Middle East and North Africa (MENA) and Gulf region are limited, making this study a valuable contribution. The median age at presentation in this study was approximately 40 years, which is consistent with other reports from the Gulf and MENA regions (9, 11-14). Macroadenomas were more common in older patients, as observed in previous regional data [10], and this may reflect their gradual progression.
Our cohort was predominantly female, which is similar to a previous study in Basra [10] and consistent with data from Oman, Turkey, and Saudi Arabia [11-13]. The female predominance among patients with NFPA may reflect earlier occurrence of health seeking behavior in women (vs. men), an increased likelihood of incidental detection during examinations for menstrual or reproductive disorders. Macroadenomas are significantly more common in men than in women, while microadenomas are more common in women. This is well supported by medical publications. A prospective study conducted at a national reference center showed that lesions >1 cm (macroadenomas) were present in 85.7% of men and 47.3% of women with NFPA (p=0.001), and male gender was significantly associated with larger tumor size (OR=1.05, p=0.049) [14]. This pattern is usually explained by late clinical presentation in men, who often seek medical care only after the onset of symptoms related to the compression effect, thus leading to diagnosis at a larger tumor size. Notably, obesity was observed in more than half of the patients with NFPA. Although NFPAs are not secretory, partial hypopituitarism (especially GH deficiency and hypogonadism) and possible disruption of hypothalamic pathways involved in appetite regulation and energy homeostasis due to the compression effect may contribute to unfavorable metabolic profiles. The observed degree of obesity suggests that this may represent an underrecognized comorbidity with clinical consequences rather than a coincidental finding, highlighting the potential need for further research into the relationship between weight and NFPAs.
In this cohort, macroadenomas were detected in the majority of patients (almost three-quarters). The predominance of macroadenomas in NFPAs likely reflects their occult, hormonally inactive course, with late clinical detection only upon manifestation of the compression effect [9].
Pituitary incidentalomas were found in approximately one in ten patients. Their prevalence can vary considerably, from one in ten cases in autopsy studies to one in twenty-five and more than one in three cases in imaging studies [15]. A 2020 multicenter study by AlMalki et al. in Saudi Arabia and the UAE found that incidental NFPAs occur in approximately one-fifth of cases [9]. In contrast, Aldahmani et al. in a 2020 cohort from the UAE discovered a higher rate, reporting incidental diagnosis in more than a third of NFPA patients [16]. These differences with our study may reflect differences in access to neuroimaging, patient referral patterns, or healthcare system structure. The comparatively lower rate of incidentalomas in our cohort may indicate a higher clinical threshold for imaging or a later presentation due to larger tumor size and symptom severity.
Chiasmal compression was observed in approximately one-third of patients, which is significantly lower than the rate reported in a 2021 study by Subramanian et al. [17]. This discrepancy may be explained by smaller tumor sizes or differences in imaging techniques. Cavernous sinus invasion was observed in approximately one-quarter of patients, as reported in the literature [18]. This finding reflects the known biological behavior of NFPAs, which typically exhibit slow but locally invasive growth.
Nearly half of the patients in our cohort underwent surgery. Transsphenoidal surgery was the most common surgical approach, consistent with the literature, which identifies it as the preferred treatment for NFPAs [7, 9, 13]. A small subgroup of patients required repeat surgeries due to incomplete resection, as well as the recurrence or regrowth of residual tumor, which is well described in the literature, including an Iranian study where 20% of patients required a second operation [19, 20].
Observation without surgical intervention was used in approximately half of the cases. It is well established that conservative treatment is an appropriate approach when surgery is not indicated [8].
Gamma Knife stereotactic radiosurgery was used in approximately one in ten patients, primarily due to residual or recurrent tumors after subtotal resection. In a study from Pakistan, 16% of patients were treated with Gamma Knife [21]. Gamma Knife is a promising treatment option in such cases [22].
Headache was the most common symptom, reported in approximately one-third of patients, followed by adrenal insufficiency in almost one-third of patients, hypopituitarism in one-quarter, and visual field defects in just under one-quarter of patients. These patterns are consistently reflected in numerous studies from the MENA region [13, 16]. Our observation that visual defects are more common in macroadenomas and in patients requiring surgery is also consistent with data from Pakistan, where Das et al. reported visual impairment and headache as key symptoms, and emphasized the need for transsphenoidal surgery, especially in patients with visual field defects [21]. Interestingly, in this study, incidental NPFAs were predominantly microadenomas, which is supported by the data of AlMalki et al., who highlighted the increasing prevalence of incidental pituitary lesions, especially microadenomas, due to the increasing number of examinations using imaging technology for unrelated complaints [9].
Our data also indicated hormone hyposecretion in larger tumors, as hypopituitarism and adrenal insufficiency were significantly more common in macroadenomas and surgical cases. This is largely due to the compressive behavior of the tumor and the concomitant interventional (vs. conservative) approach. In one study from Iran, hypopituitarism was observed in half of patients with macroadenomas [20], while in a study from Pakistan, adrenal insufficiency was documented in approximately half of the cases [21]. These findings are further supported by data from Saudi Arabia [9]. In a study by Mansour et al. in Basra, macroadenomas were also prevalent, and the authors reported that visual field defects were the most common complaint, with the decision for surgical intervention based on visual field defects and pituitary dysfunction [10]. Collectively, these data from diverse populations in the MENA region support the association between tumor size and clinical severity, emphasizing the importance of early imaging, hormonal screening, and timely intervention to mitigate complications in patients with NFPA.
Hyperprolactinemia was observed in approximately half of the patients. This is an important association with NFPA in the historical context [23, 24]. Hyperprolactinemia due to a nonfunctioning microadenoma may be explained by the fact that even small pituitary microadenomas can elevate prolactin levels by disrupting portal blood flow between the hypothalamus and pituitary gland. This may help explain why prolactin levels do not always correlate closely with tumor size in NFPA. One factor contributing to the development of ESS is increased pressure within the sella turcica (intrasellar pressure), which can disrupt normal hormone production by both the hypothalamus and the anterior pituitary gland. This disruption can lead to hormonal imbalances, including elevated prolactin levels [25].
ESS has been observed in approximately one in five patients and can potentially result from surgery or pituitary apoplexy. A comprehensive assessment of pituitary function is crucial in the diagnosis of ESS [26]. Arginine vasopressin deficiency was observed in approximately one in fifteen patients, which is within the range of one in forty-five to one in ten reported in large studies [27, 28]. Cranial nerve palsies, particularly hemianopia, were observed in approximately one in thirty-three patients, which is slightly lower than the one in twenty to one in six reported in the literature [29]. The lower prevalence may be explained by variability in tumor growth pattern and differences in patient referral patterns or thresholds for ocular assessment.
CSF rhinorrhea was observed in one in seventy cases, which is comparable to the 2021 study by Thakur et al., who reported a CSF leak rate of one in fifty. Meningitis was virtually uncommon in our cohort, reflecting the low incidence of this complication due to recent improvements in surgical treatment [27]. Pituitary apoplexy was observed in approximately one in twenty cases, which is consistent with previous reports, where the incidence of apoplexy in pituitary adenomas ranges from one in fifty to one in ten, with the majority of cases occurring in NFPAs [30]. Residual tumor was detected in 23.8% of all patients, and 45.7% of them underwent surgery. This is comparable to published data, where 57% of patients had postoperative residual tumor [19].
Regional differences between our results and data from Oman, Saudi Arabia, the UAE, and other MENA countries should be interpreted in the context of underlying socioeconomic and healthcare system differences. Differences in access to specialized endocrinology and neurosurgical services, patient referral pathways, and availability of routine hormonal testing and neuroimaging may influence the timing of diagnosis, tumor size at presentation, and the detection of concomitant hormonal disorders. Furthermore, population-level differences in metabolic risk factors, including obesity prevalence and lifestyle, may contribute to variations in the reported clinical profiles.
Limitations of the study
This study has several limitations. First, its single-center retrospective design may limit the generalizability of the results, as patient characteristics, referral patterns, diagnostic practices, and treatment strategies at our tertiary center may not fully reflect the situation at other institutions or regions. Furthermore, retrospective data collection may result in incomplete documentation and potential selection bias, which could have influenced the observed clinical and radiological characteristics. Therefore, our results should be considered primarily as a reflection of local practice, highlighting the need for multicenter prospective studies to confirm these findings. Additionally, the lack of randomized treatment groups and limited long-term follow-up data may have impacted conclusions regarding treatment efficacy and recurrence. Finally, we were unable to determine whether hypopituitarism developed pre- or postoperatively due to the study design and missing data in some cases where patients were referred to our center post-operatively.
Conclusion
This study provided important information on the presentation and treatment of NFPA. Macroadenomas were the most common, with transsphenoidal surgery being the treatment of choice. High rates of obesity and hyperprolactinemia indicated the need for further research to explore their potential association with NFPA. Future prospective studies with longer follow-up periods are needed to refine treatment strategies and improve patient outcomes.
Acknowledgments
The authors express their sincere gratitude to the patients whose data were used in this retrospective study, as well as to the medical staff at FDEMC for their invaluable support in data collection, anthropometric measurements, and blood sample analysis, utilizing the expertise of qualified laboratory personnel.
Author contributions
Musaab A. Alhussein conceived the study concept, processed the data, conducted the formal analysis, developed the methodology, created the visualizations, and wrote the initial draft.
Ammar M. Almomin processed the data, conducted the research, managed the project administration, and contributed to reviewing and editing the manuscript.
Abbas A. Mansour provided supervision, secured resources, reviewed the research portion of the study, reviewed and edited the manuscript, and provided final approval.
All authors have reviewed and approved the final version of the manuscript and agreed to be accountable for all aspects of this study.
AI statement
In preparing this manuscript, the authors used an artificial intelligence-powered language editing tool (ChatGPT, OpenAI) solely for editing and paraphrasing the text to improve its clarity and readability. The scientific content, data interpretation, and conclusions were developed entirely by the authors. All results were carefully reviewed, edited, and approved by the authors, who take full responsibility for the integrity and accuracy of the manuscript.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
The study received no external funding.
Ethical approval
This study was conducted in accordance with the ethical standards of the FDEMC Research Committee and in accordance with the principles set forth in the Declaration of Helsinki (1964) and its subsequent amendments or comparable ethical guidelines. Approval to conduct the study was obtained from the FDEMC Ethics Committee under number 56/35/22 dated June 18, 2025. The study was retrospective and based solely on anonymized data obtained from existing medical records, without direct contact with participants or any deviations from routine clinical practice. Accordingly, the requirement for written informed consent was waived by the Ethics Committee, as formal consent is not required for this type of study.
- Dolecek TA, Propp JM, Stroup NE, Kruchko C. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2005-2009. Neuro Oncol 2012; 15(5): 646-647. https://doi.org/10.1093/neuonc/nos218.
- Ezzat S, Asa SL, Couldwell WT, Barr CE, Dodge WE, Vance ML, et al. The prevalence of pituitary adenomas: A systematic review. Cancer 2004; 101(3): 613-619. https://doi.org/10.1002/cncr.20412.
- Ntali G, Wass JA. Epidemiology, clinical presentation and diagnosis of non-functioning pituitary adenomas. Pituitary 2018; 21(2): 111-118. https://doi.org/10.1007/s11102-018-0869-3.
- Lamback EB, Wildemberg LE, Gadelha MR. Current opinion on the diagnosis and management of non-functioning pituitary adenomas. Expert Rev Endocrinol Metab 2021; 16(6): 309-320. https://doi.org/10.1080/17446651.2021.1988851.
- Whyte E, Nezu M, Chik C, Tateno T. Update on current evidence for the diagnosis and management of nonfunctioning pituitary neuroendocrine tumors. Endocrinol Metab (Seoul) 2023; 38(6): 631-654. https://doi.org/10.3803/enm.2023.1838.
- Hussein Z, Slack RW, Marcus HJ, Mazomenos EB, Baldeweg SE. Post-operative medium- and long-term endocrine outcomes in patients with non-functioning pituitary adenomas-machine learning analysis. Cancers (Basel) 2023; 15(10): 2771. https://doi.org/10.3390/cancers15102771.
- Fernandez-Balsells MM, Murad MH, Barwise A, Gallegos-Orozco JF, Paul A, Lane MA, et al. Natural history of nonfunctioning pituitary adenomas and incidentalomas: A systematic review and metaanalysis. J Clin Endocrinol Metab 2011; 96(4): 905-612. https://doi.org/10.1210/jc.2010-1054.
- Rikvold SD, Pedersen MB, Andreassen M, Krogh J. Natural history of non-functioning pituitary adenomas: A systematic review and meta-analysis. Horm Metab Res 2023; 55(7): 443-451. https://doi.org/10.1055/a-2096-1340.
- AlMalki MH, Ahmad MM, Brema I, AlDahmani KM, Pervez N, Al-Dandan S, et al. Contemporary management of clinically non-functioning pituitary adenomas: A clinical review. Clin Med Insights Endocrinol Diabetes 2020; 13: 1179551420932921. https://doi.org/10.1177/1179551420932921.
- Mansour AA, Alhamza AHA, Almomin A, Zaboon IA, Alibrahim NTY, Hussein RN, et al. Spectrum of pituitary disorders: A retrospective study from Basra, Iraq. F1000Res 2018; 7: 430. https://doi.org/10.12688/f1000research.13632.2.
- Duran ID GN, Berker D, Guler S. Is there a gender difference in clinically nonfunctional pituitary adenomas? Endocrine Abstracts 2017; 49: EP977. https://doi.org/10.1530/endoabs.49.EP977.
- Hussein SH, Wahedi TS, Johani NA, Hakami YA, Alzahrani K, AlMalki MH. Clinical and epidemiological characteristics of pituitary tumours in a single centre in Saudi Arabia. Hormones (Athens) 2018; 17(2): 261-267. https://doi.org/10.1007/s42000-018-0030-8.
- Al Futaisi AM, Al Marzouqi AM, Al Abri MA, Al Riyami MZ. Pituitary adenoma prevalence and characteristics of Omani patients: A single center experience. Oman Med J 2024; 39(1): e589. https://doi.org/10.5001/omj.2024.44.
- Di Somma C, Scarano E, de Alteriis G, Barrea L, Riccio E, Arianna R, et al. Is there any gender difference in epidemiology, clinical presentation and co-morbidities of non-functioning pituitary adenomas? A prospective survey of a National Referral Center and review of the literature. J Endocrinol Invest 2021; 44(5): 957-968. https://doi.org/10.1007/s40618-020-01379-2.
- Freda PU, Beckers AM, Katznelson L, Molitch ME, Montori VM, Post KD, et al. Pituitary incidentaloma: An endocrine society clinical practice guideline. J Clin Endocrinol Metab 2011; 96(4): 894-904. https://doi.org/10.1210/jc.2010-1048.
- Aldahmani KM, Sreedharan J, Ismail MM, Philip J, Nair SC, Alfelasi M, et al. Prevalence and characteristics of sellar masses in the city of Al Ain, United Arab Emirates: 2010 to 2016. Ann Saudi Med 2020; 40(2): 105-112. https://doi.org/10.5144/0256-4947.2020.105.
- Subramanian V, Lee RSM, Howell S, Gregson S, Lahart IM, Kaushal K, et al. Non-functioning pituitary macroadenomas: factors affecting postoperative recurrence, and pre- and post-surgical endocrine and visual function. Endocrine 2021; 73(2): 407-415. https://doi.org/10.1007/s12020-021-02713-1.
- Ajlan A, Achrol AS, Albakr A, Feroze AH, Westbroek EM, Hwang P, et al. Cavernous sinus involvement by pituitary adenomas: Clinical implications and outcomes of endoscopic endonasal resection. J Neurol Surg B Skull Base 2017; 78(3): 273-382. https://doi.org/10.1055/s-0036-1598022.
- Charleux T, Vendrely V, Huchet A, Trouette R, Ferriere A, Tabarin A, et al. Management after initial surgery of nonfunctioning pituitary adenoma: Surveillance, radiotherapy or surgery? Radiat Oncol 2022; 17(1): 165. https://doi.org/10.1186/s13014-022-02133-z.
- Najmaldin A, Malek M, Madani NH, Ghorbani M, Akbari H, Khajavi A, et al. Non-functioning pituitary macroadenoma: Surgical outcomes, tumor regrowth, and alterations in pituitary function-3-year experience from the Iranian Pituitary Tumor Registry. Hormones (Athens) 2019; 18(2): 197-205. https://doi.org/10.1007/s42000-019-00109-5.
- Das B, Batool S, Khoja A, Islam N. Presentation, management, and outcomes of nonfunctioning pituitary adenomas: An experience from a developing country. Cureus 2019; 11(9): e5759. https://doi.org/10.7759/cureus.5759.
- De Nigris Vasconcellos F, Vilela MAD, Garcia Torrico F, Scalise MA, Vargas VPS, Mendieta CD, et al. Stereotactic radiosurgery for recurrent/residual nonfunctioning pituitary adenoma: A single-arm systematic review and meta-analysis. Acta Neurochir (Wien) 2024; 166(1): 392. https://doi.org/10.1007/s00701-024-06296-4.
- Fleseriu M, Bodach ME, Tumialan LM, Bonert V, Oyesiku NM, Patil CG, et al. Congress of Neurological Surgeons systematic review and evidence-based guideline for pretreatment endocrine evaluation of patients with nonfunctioning pituitary adenomas. Neurosurgery 2016; 79(4): E527-E529. https://doi.org/10.1227/neu.0000000000001387.
- Zhang F, Huang Y, Ding C, Huang G, Wang S. The prevalence of hyperprolactinemia in non-functioning pituitary macroadenomas. Int J Clin Exp Med 2015; 8(10): 18990-18997. https://pubmed.ncbi.nlm.nih.gov/26770524.
- Park SS, Kim JH, Kim YH, Lee JH, Dho YS, Shin CS. Clinical and radiographic characteristics related to hyperprolactinemia in nonfunctioning pituitary adenomas. World Neurosurg 2018; 119: e1035-e1040. https://doi.org/10.1016/j.wneu.2018.08.068.
- Ghatnatti V, Sarma D, Saikia U. Empty sella syndrome – Beyond being an incidental finding. Indian J Endocrinol Metab 2012; 16(Suppl 2): S321-S323. https://doi.org/10.4103/2230-8210.104075.
- Thakur JD, Corlin A, Mallari RJ, Yawitz S, Eisenberg A, Sivakumar W, et al. Complication avoidance protocols in endoscopic pituitary adenoma surgery: a retrospective cohort study in 514 patients. Pituitary 2021; 24(6): 930-942. https://doi.org/10.1007/s11102-021-01167-y.
- Nemergut EC, Zuo Z, Jane JA Jr, Laws ER Jr. Predictors of diabetes insipidus after transsphenoidal surgery: a review of 881 patients. J Neurosurg 2005; 103(3): 448-454. https://doi.org/10.3171/jns.2005.103.3.0448.
- Kim SH, Lee KC, Kim SH. Cranial nerve palsies accompanying pituitary tumour. J Clin Neurosci 2007; 14(12): 1158-1162. https://doi.org/10.1016/j.jocn.2006.07.016.
- Briet C, Salenave S, Bonneville JF, Laws ER, Chanson P. Pituitary apoplexy. Endocr Rev 2015; 36(6): 622-645. https://doi.org/10.1210/er.2015-1042.
Received 6 October 2025, Revised 14 January 2026, Accepted 5 March 2026
© 2025, Russian Open Medical Journal
Correspondence to Musaab A. Alhussein. E-mail: musaab.ashkar@yahoo.com.